Ravn
Senior Member (Voting Rights)
Provisionally accepted 26 Feb 2019, full text soon
Chronotropic incompetence: an overlooked determinant of symptoms and activity limitation in myalgic encephalomyelitis/chronic fatigue syndrome?
Davenport et al
Chronotropic incompetence: an overlooked determinant of symptoms and activity limitation in myalgic encephalomyelitis/chronic fatigue syndrome?
Davenport et al
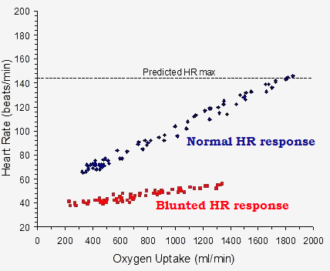
https://www.frontiersin.org/articles/10.3389/fped.2019.00082/abstractPost-exertional malaise (PEM) is the hallmark clinical feature of myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). PEM involves a constellation of substantially disabling signs and symptoms that occur in response to physical, mental, emotional, and spiritual over-exertion. Because PEM occurs in response to over-exertion, physiological measurements obtained during standardized exertional paradigms hold promise to contribute greatly to our understanding of the cardiovascular, pulmonary, and metabolic states underlying PEM. In turn, information from standardized exertional paradigms can inform patho-etiologic studies and analeptic management strategies in people with ME/CFS. Several studies have been published that describe physiologic responses to exercise in people with ME/CFS, using maximal cardiopulmonary testing (CPET) as a standardized physiologic stressor. In both non-disabled people and people with a wide range of health conditions, the relationship between exercise heart rate (HR) and exercise workload during maximal CPET are repeatable and demonstrate a positive linear relationship. However, s maller or reduced increases in heart rate during CPET are consistently observed in ME/CFS. This blunted rise in heart rate is called chronotropic incompetence (CI). CI reflects an inability to appropriately increase cardiac output because of smaller than expected increases in heart rate. The purposes of this review are to (1) define CI and discuss its applications to clinical populations; (2) summarize existing data regarding heart rate responses to exercise obtained during maximal CPET in people with ME/CFS that have been published in the peer-reviewed literature through systematic review and meta-analysis; and (3) discuss how trends related to CI in ME/CFS observed in the literature should influence future patho-etiological research designs and clinical practice.
")