Those who went on to meet ME/CFS case definitions had more anxiety, depression, dysfunctional coping, perceived stress etc. So I assume that proponents of the psychosomatic view on ME/CFS will argue that these findings support their theory
Perhaps, but for a young adult, anxiety and depression would be totally appropriate if you had an infection and did not recover, could not possibly go dancing and socializing at night, and had trouble studying- the prolonged illness state is unexpected especially at this stage of their lives. Uncertainty and lingering symptoms that restrict living a full life while not getting answers in health care would generate anxiety and depression.
Unfortunately, from the facebook Long-COVID groups, patients with Long-COVID also experience anxiety and depression due to their circumstances, not being believed being one major cause, but also uncertainty in regards to their future.
I sometimes think it might be helpful to indicate that it was only recently that the Mayo clinic removed CBT and GET from their website, and that the UK fanatics might originally have obtained the basics, if not the particulars, of the treatment from the US. It seems rather divisive to pretend it was all the UK psychiatrists' idea.
Well, I've written about Mayo multiple times, and have repeatedly blasted the CDC for avoiding its public health responsibilities in this domain. However, the UK cabal has been the primary driver of this movement in the literature and in research, along perhaps with the Dutch and the Danes--even if the use of the term CFS for the Tahoe outbreak inspired them on this front.
Yes, but all they did was to develop the concept of illness behaviour which was already developed in the US. All their ideas are already to be seen in the McHugh and Vallis book. I am not making a point about the US. I am sure there was a great deal of cross fertilisation of ideas; in the UK Shepherd was clearly an exponent of such opinions, but they are less well known, and it appears that before writing his 1966 paper on illness behaviour Mechanic spent time at the Maudsley and acnowledges the assistance of JK Wing.
It should also be borne in mind that in the 1995 Surawy et al paper (al including Sharpe) the advice of Beck was acknowledged. They could never have done this alone.
Sure, that's a reasonable perspective, although I might quibble with the phrase "all they did"--that covers a lot of damage!! The distinction between illness and disease has also been popular in medical anthropology circles in the US for decades, so it's nothing new from Michael Sharpe. But when it comes to applying general theories to this particular illness or cluster of illnesses, the UK group grabbed that and ran with it for the last 30 years.
Those who went on to meet ME/CFS case definitions had more anxiety, depression, dysfunctional coping, perceived stress etc. So I assume that proponents of the psychosomatic view on ME/CFS will argue that these findings support their theory.
Hats off to Lenny Jason and colleagues for pulling off and a huge and significant study.
This is the first truly prospective study of post-infectious ME/CFS. The importance of prospective studies is that measuring what happens before the illness starts allows researchers to identify causal factors. Most studies in ME/CFS can only find associations with illness, which can’t distinguish cause from effect.
This was a huge study. 4700 students were enrolled between March 2014 and June 2018. Most of them were in their first year and about half of each incoming class enrolled in the study. More than 95% of those who enrolled completed the surveys (nine of them, I think) and gave a blood sample.
The paper says that students were compensated fortaking part, which looks like a smart move, because these participation rates are incredible.
Out of this huge cohort of 4500 students, 238 (5%) developed infectious mononucleosis (glandular fever) by the end of June 2019. 55 of these (23%) met at least one of the criteria for ME/CFS are (CCC, Fukuda and IOM). 20 students meant at least 2 criteria and were classified as severe (@Andy no further qjustification for this was given).
157 students no longer had symptoms at six months and were classified as recovered.
Key results
Comparing those with mono who recovered with those who developed ME/CFS, there appear to be two important results from this study:
1. There are no siginficant differences between the two groups on the measured psychological factors of stress, coping, anxiety or depression at baseline. That seriously undermines psychosocial theories of the illness. If they need undermining any further.
2. "In a previous study, we identified mononucleosis severity as a risk factor for severe ME/CFS. That relationship was found in the present analysis as well (p = 0.04; data not shown)". and the P value isn't impressive but it also ties in with findings from the Dubbo study. And with Peter White's infectious mono study, which found that days of bedrest predicted CFS. They don't say how severity was measured.
Otherwise, not so much to see, I fear
Based on my first reading of the paper, there is otherwise not a huge amount here. There are some differences but I'm not sure if the authors have corrected sufficiently for the very high number of comparisons(e.g they use results from 12 different scales but use a p value of 0.01). And in any case the differences appear to be quite small even if they are significant.
I'd be very to know if @Jonathan Edwards thinks cytokine differences given in table 3 are likely to mean very much.
Some issues to discuss
This situation is disappointing. There are a few methodological issues that may or may not be relevant. I would appreciate the views of others.
1. Data and blood samples were taken "within six weeks of diagnosis". That strikes me as quite a wide window and I thought it was much shorter for both Dubbo and the Peter White study. This raises the possibility that, for at least some people, the data and blood sample were collected after the main action was over.
2. I am not convinced that the threshold for "substantial reduction in activities# was especially strong.
Surprisingly, the study does not use the SF36 Physical Functioning PF scale, which is the scale used by most researchers in diagnosis. Instead, the authors define substantial reduction as "scoring at or below at least two of three cut-offs on the SF 36: role physical <= 50, social functioning l<= 62.5, and vitality <= 35.
Also, this study uses the DePaul symptom questionnaire and its definition of PEM. There are reasons to question whether that actually captures PEM, with the risk that sweeps people into a diagnosis that perhaps shouldn't be there.
However, all diagnosed cases did have a medical exam and physical and psychological assessment.
Certainly, the very high proportion of people with IM developing ME/CFS at six months (23%) is surprisingly.
3. For the non-severe ME/CFS cases (i.e. meeting only one criteria, which the paper says was almost always Fukuda) the increases in fatigue and DSQ scores from baseline are modest.
DSQ symptom scores increased from 17 at baseline to 20 at six months, while the fatigue score increased from 33 to 39. The severe ME/CFS scores showed a bigger incremental increase, but it still wasn't huge. Certainly, I think these small incremental increases cast some doubt on the validity of the single-criteria-meeting standard ME/CFS group.
Okay, I am done.
Added: apologies for not quoting people's contributions; not easy on an iphone and trying to avoid triggering the next bloody migraine with too much screen use.
Many college students fully recover from infectious mononucleosis (which is almost always caused by Epstein-Barr virus) within 1-6 weeks, but some go on to develop chronic fatigue syndrome, also called myalgic encephalomyelitis (ME/CFS). A longitudinal study from DePaul University and Northwestern University followed 4,501 college students to examine risk factors that may trigger longer illness. The research appears in the journal Clinical Infectious Diseases and was funded by the National Institute of Allergy and Infectious Diseases.
The researchers discovered that people who developed ME/CFS had more physical symptoms and immune irregularities at baseline. The participants did not start with more psychological symptoms, such as stress, depression, anxiety or abnormal coping.
"It turns out that our results suggest those more psychiatric variables were not predictors of who got mono and stayed sick and who got mono and did not stay sick," Jason said.
According to Dr. Lily Chu, vice president of the International Association for Chronic Fatigue Syndrome/Myalgic Encephalomyelitis, the misconception that ME/CFS is caused by psychological reasons has persisted for decades. This study adds to the evidence that ME/CFS is not a psychiatric or psychological condition, she said.
Has anyone pointed out that this appears to be a direct contradiction of the "findings" of Imboden, Canter and Cluff relating to chronic brucellosis and Asian flu, and upon which the BPS model for CFS was partly based? As Fauci seems to have supported Straus over the issue who are we to believe?
article: Study examines risk factors for developing ME/CFS in college students after infectious mononucleosis
Many college students fully recover from infectious mononucleosis (which is almost always caused by Epstein-Barr virus) within 1-6 weeks, but some go on to develop chronic fatigue syndrome, also called myalgic encephalomyelitis (ME/CFS). A longitudinal study from DePaul University and Northwestern University followed 4,501 college students to examine risk factors that may trigger longer illness. The research appears in the journal Clinical Infectious Diseases and was funded by the National Institute of Allergy and Infectious Diseases.
Previous retrospective studies found that risk factors for developing ME/CFS after catching mono included preexisting physical symptoms and the number of days spent in bed, according to co-principal investigators Leonard A. Jason, professor of psychology at DePaul University; and Dr. Ben Z. Katz, a professor of pediatrics at Northwestern University Feinberg School of Medicine and a pediatric infectious disease specialist at Ann & Robert H. Lurie Children's Hospital of Chicago.
Coming back at this paper. Participants were assessed before mononucleosis (time1) during mono (time2) and 6 months after mono (time 3).
The authors reported no statistically significant result at time 1 for anxiety (BAI questionnaire) and depression (BDI-II) but I think this is because they arbitrarily split the ME/CFS group into two. I believe that if the 49 ME/CFS patients were taken as a whole and compared to the recovered control group, many of the baseline values would show a statistically significant difference as the difference are quite obvious (see calculations below).
The main finding seems to be that patients who reported more fatigue, depression, stress, anxiety and other DSQ-symptoms before getting mono were likely to be diagnosed with ME/CFS, 6 months after mono. One interpretation could be that if your baseline level of symptoms is already high, you are more likely to meet ME/CFS diagnostic criteria after getting a serious infection.
When testing for predictors of ME/CFS it might therefore be important to control for these baseline symptoms in regression analysis or exclude patients who were already fatigued. I believe this is the approach that the Lifelines cohort used and they found that anxiety and depression were not a predictor of (self-reported) ME/CFS. One can debate what is the most suitable approach because it is quite an interesting finding in itself that baseline symptoms are a predictor. A lot depends on what you put as variables in the regression analysis. It is quite unfortunately that we have so little longitudinal data and that none of the raw data is publicly available.
Calculations and estimations
Here are my calculations. For the BAI-anxiety questionnaire at timepoint 1, I calculated the weighted mean, weighted standard deviation (using this formula) and sample size of the two ME/CFS groups combined.
Mean = 8.33
Sd = 7.44
N = 49
For the control group the values are:
Mean = 3.88
Sd = 4.57
N = 60
When I did a independent t-test for this difference, I got a significant result (t = 3.65, p = 0.00047).
Similarly for the BDI-II (depression) at time 1, the combined ME/CFS groups looks like this:
Mean = 9.86
Sd = 7.71
N = 49
For the control group the values are:
Mean = 5.43
Sd = 4.50
N = 60
Here I get a t-value of 3.56 and p-value of 0.00066.
The result for the PSS-stress questionnaire gave the following data. For the combined ME/CFS group:
Mean = 6.92
Sd = 3.14
N = 49
For the control group the values are:
Mean = 5.58
Sd = 2.74
N = 60
This gave a t-value of 2.34 and a p-value of 0.021.
I'm concerned that assessment of "substantial reduction in activities" has included those too mild to have ME/CFS, which would weaken the study if it is the case. The authors used thresholds and scales validated in an earlier study that compared accuracy of CFS cases vs negative controls, which isn't appropriate for ruling out people recovering from IM who do not have ME/CFS.
"[For diagnosis with ME/CFS,] participants needed to experience substantial reductions in occupational, educational, or personal activities [28], by scoring at or below at least 2 of the 3 following subscale cutoffs on the SF-36: Role Physical of 50 or less, Social Functioning of 62.5 or less, and Vitality of 35 or less." The scales and thresholds came from this 2010 study. It used three questions from the SF36 questionnaire (RAND SF36 questionnaire): Role Physical, Social Functioning and Vitality. None of these is ideal, though would give good separation between true ME/CFS cases and healthy controls.
This study takes data from Jason's 1999 Prevalence paper and a separate tertiary sample and assesses which of the eight SF36 questionnaire measures best separate diagnosed cases from controls.
1999 study: 32 CFS cases and 47 controls.
Tertiary care sample: 114 cases (baseline data from an intervention trial) - no controls.
The controls are described as "composed of individuals selected randomly from those 18,260 screened negatives (groups included participants with no reported prolonged or chronic fatigue) [of which] the physician review team identified 47 individuals who were medically worked up and found not to have CFS."
As the overall sample was recruited through random dialing of Chicago numbers, this group should be broadly representative of the population, so pretty healthy. Unfortunately, this paper gives no further details about their health.
The study selected the Vitality, Role Physical and Social Functioning scales because they gave the best separation with their (probably pretty healthy) controls. Most of the Qs only have a few rungs on the scale: RP only has 5 levels (All no through to All Yes), SF has 11. Vitality has more, but doesn't measure activity levels directly, and there are better measures of fatige). Having fewer possible levels is good for picking up big differences like healthy vs sick. But not well suited to more subtle differences (having a mild vs more severe illness).
In contrast, the Physical Functioning scale, which is more widely used for functioning, has 21 levels so is better suited for detecting smaller differences.
Role Physical
During the past 4 weeks, have you had any of the following problems with your work or other regular daily activities as
a result of your physical health? 0-100 score. Yes/No answers, scoring 25/0.
Cut down the amount of time you spent on work or other activities?
Accomplished less than you would like?
Were limited in the kind of work or other activities?
Had difficulty performing the work or other activities (for example, it took extra effort?
The threshold for reduced activities 50 or less, so two or more "Nos" is sufficient, which probably anyone who is unwell or still recovering from IM would say, whiles healthy people would readily score 75 or 100. This is the most problematic scale as almost anyone sick would qualify, meaning only one of the following 2 scale thresholds has to be met to meet the study criterion for reduced activity.
Social Functioning
This consists of two very similar questions:
During the past 4 weeks, to what extent has your physical health or emotional problems interfered with your normal social activities with family, friends, neighbors, or groups?
This scored 0-50, where 50 signals the best health: Not at all=50; Slightly=37.5; Moderately=25; Quite a bit=12.5; Extremely=0.
An almost identical question later in the survey asks about "how much of the time" rather than "to what extent" ans is scored in a similar way. The scores from the two questions are added to give a 0-100 score.
The threshold for reduced activity is 62.5 or less, so someone who is moderately affected (or worse) a little of the time (or more often) would meet the Social Functioning "redcued activity" threshold . Again, this would split healthy controls from those with ME/CFS, but not be good at excluding those with other health issues.
Vitality
Four questions designed to assess energy levels and fatigue. These aks respondents how much of the time during the past four weeks:
Did you feel full of life?
Did you have a lot of energy?
Did you feel worn out?
Did you feel tired?
Each question is scored 0-25 for options where the highest score means better health:
All of the time; Most of the time; A good bit of the time; Some of the time; A little bit of the time; or None of the time.
The threshold is a score of 50 or less. So if you felt full of life and had a lot of energy a little of the time (5+5), and felt worn out a good bit of the time (15) and tired some of the time (10), you woul score 45 points and meet the threshold.
Also, Vitality is a measure of energy and fatigue, not activity, which is being assessed here. If they wanted to measure fatigue, the FSS, which the study uses, would be a better option.
Overall, it looks pretty easy for someone with mediocre health to meet the threshold for two or more questions, if they are unwell, say slow to recover from IM, but don't have ME/CFS.
The next post (which might not happen for some time) will look at the overal fatigue and health scores fto try to judge how ill the different groups are (recovered vs ME/CFS vs S-ME/CFS).
Summary: Do the cases selected in the study appear to be severe enough to qualify for ME/CFS?
For S-ME/CFS yes. But it's likely that many with "ME/CFS" do not: as they seem to have reasonable overall health, a significant minority don't have even have moderate fatigue, and the group only shows a small increase in symptoms from baseline.
---
The previous post argued that the SF36 questions and thresholds used in this study would pull in those who hadn't properly recovered from IM, but weren't ill enough to have ME/CFS. This post looks at the data to see if it is the case.
The study doesn't give any data on reduction in activity, with no data on the three SF36 subscales used: Role Physical, Social Functioning and Vitality.
However, it gives us data that does help gauge severity: the SF36 Physical Component Summary, the FSS fatigue score, and the DSQ symptoms scores.
SF36 Physical Component Summary (PCS)
This is a complex measure, you might want to skip this and go to the data image below, but iti is not intuitive to understand.
The PCS and Mental Component Summary aim to simplify interpretation of SF36 scores from the 8 different subscales. Using factor analysis, they identified a mental and physical health summary, which is said to capture 80-85% of the variance.
The PCS is calculated from the Role Physical subscale, the Physical Functioning subscale (which is widely used to assess ME/CFS activity levels), and the bodily pain subscale and a general health subscale. It's a weighted calculation, and is much broader than just activity levels.
Note that Social Functioning and Vitality subscales are part of the mental health MCS, not PCS – another reason to suggest these are not good measures for assessing activity levels.
Note PCS uses "normalised" scores, which are not intuitive. A score of 50 = same score as the average for the US population.. A score of 40, ten points lower, might not seem much but it equals one SD lower, a big effect. Put another way, a score of 40 means 84% of the US reference population has a better PCS than this. Similarly, a score of 60 is1 SD above the mean, so better than 84% of the US population.
SF-36 norm-based scoring (NBS)
transforms raw survey responses into standardized scores with a mean of 50 and a standard deviation (SD) of 10, based on the general U.S. population. This method allows for easier comparison across the 8 health domains, with scores above 50 indicating better-than-average health and below 50 indicating poorer-than-average health. Key Aspects of SF-36 Norm-Based Scoring
Standardization: Unlike 0–100 scoring, NBS sets the general population mean at 50 and SD at 10, facilitating direct comparisons between different diseases, populations, or interventions.
Interpretation: A score of 50 represents the average, 40 is one SD below average, and 60 is one SD above, making it easy to identify if a group is above or below the norm.
Components: NBS is applied to the eight subscales (Physical Functioning, Role-Physical, Bodily Pain, General Health, Vitality, Social Functioning, Role-Emotional, Mental Health) and the two summary measures: Physical Component Summary (PCS) and Mental Component Summary (MCS).
Advantages: NBS simplifies the interpretation of results and is generally recommended over0–100 scoring for analyzing, interpreting, and comparing health outcomes.
Data Requirements: QualityMetric provides the necessary, certified algorithms for this scoring, often used with the SF-36v2 survey.
The data shows the the S-ME/CFS group PCS score is 1 SD below its baseline score, a large effect size. By comparison, the ME/CFS group only drops by 0.5 SD, a moderate effect size. I'm not sure that modest reduction in health is compatible with ME/CFS.
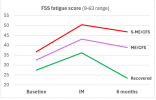
We see a similar pattern with the fatigue scores:
The FSS is a nine-item scale with each question scored from 1-7, where 7 represents the worst fatigue. giving a score range of 9-63. A score of 36 (equivalent to a score of 4 on each of 9 questions) is often used the threshold for moderate fatigue. This score is marked in grey on the graph below.
Note that mean score of the S-ME/CFS group is 36.7, already achieving the thresholdat basline (so, if normally distributed, half will have scores above the threshold, half below). The ME/CFS group is not far below at 32.6, adn the recovery group has a score of 27.4 at baseline, equivalent to a score of 3/7 on every fatigue question. That's quite high.
For ME/CFS, the mean score is 38.9, with an SD of 8.6, indicating about 30%-40% of people in the group have fatigue below the moderate fatigue threshold of 36.
Perhaps a student lifestyle contributes to these relatively high scores, though the DSQ symptom scores, below, indicate less than perfect baseline health for at least the S-ME/CFS group.
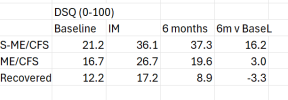
DSQ,
The DSQ measures symptom frequency and severity, and is scaled from 0-100. Note that it covers many symptoms, especially for Canadian criteria, and it's likely that few people score for most of the measured symptoms.
The pattern appears to be that the S-ME/CFS is severe enough to qualify for ME/CFS, but are certainly not severe. It is the only group where the DSQ score goes up during acute IM and stays high at 6 months. While the simple ME/CFS group (meeting only one case criterion) is midway between recovered and the S-ME/CFS group. It's DSQ score increases from 16.7 at baseeline to 19.6 at 6 months = +3 , caompared iwth +16 for S-CFS.
The significant DSQ baseline score symptom score for the ME/CFS group probably makes it relatively easy to meet Fukduda's list of generic symptoms, given that none a mandatory.
I think these scores suggest that the ME/CFS is not that ill, certainly compared with baseline, and may not be fatigued enough or have poor enough health to credibly count as ME/CFS.
More on this is the next post. Which I promise will be shorter.
Trying to work out the make up of the ME/CFS group (I)
The story so far: Are the measures used to assess reduced activity levels necessary for ME/CFS appropriate?
As the two posts above show, they don't seem suitable to separate those with ME/CFS from those those not yet fully recovered from IM but without ME/CFS. Morover, theyhave pulled in people to the ME/CFS group who don't have moderate fatigue, appear in reasonable health (vs baseline) and had plenty of symptoms at baseline that might make it easy to meet the Fukuda criteria, especially if they picked up a few more symptoms due to not recovering fully from IM.
To intepret these results, it's useful to look at the rate of ME/CFS after IM for this study:
S-ME/CFS = 8%
ME/CFS = 15%
All ME/CFS = 23%
This looks out of line with other IM and post-infectious studies:
Dubbo (Hickie, 2006) 12% (Some EBV, but mostly post Q-fever and Ross River Virus in adults) Katz, 2009 13% (adolescents) Pedersen, 2019, 12% (adolesents)
So S-ME/CFS looks much too low on its own at 8%, while in combimation with simple ME/CFS the total figure is much too high (roughly double that of other studies).
What might the "ME/CFS" group include?
The implication of these headline figures is that the S-ME/CFS looks sound, while the ME/CFS group contains some true ME/CFS and more non-ME/CFS cases. This was raised on the recent thread about the follow-up paper to this study:
There's perhaps the idea that what they call "severe-ME/CFS" would represent what we would call ME/CFS and the other is more akin to post-viral fatigue but I'm not even sure about that (for example Fukuda can also include for example people with MS or depression and of course those disease are also not mild as the authors would say).
Looking at the data in this post and the two before it, my current take is that the ME/CFS group (15% of all IM cases) contains those with true ME/CFS. Let's say 4% of total IM cases, giving a total ME/CFS rate of 12% (8% S-ME/CFS+4%)
Those with post viral fatigue syndrome (PVFS), since they have moderate fatigue + non-fatigue symptoms captured by Fukuda. Let's say 5%.
Those with somethig else who don't have moderate fatigue. Say 6% of all IM cases, about 40% of the ME/CFS group.
This might include MS, but I doubt there would be more than a tiny number post-IM. The derpression scores indicate mild depression only. I don't have any better ideas, but it might relate to baseline heatlh issues picked up by the clinical examination.
I'd appreciate comments on the above post.
PS. We can probe the Jason study because it provides so much data, and I'm going to so much trouble because the study design is so good, and I think it's findings are very important. These findings prompted me to go back to the other pst-infectious studies I quote above, and I found the results there are not quite as clear cut as it seems. But that is for another day.
That looks a fair analysis. From my own experience of 6 months of feeling not well after IM I think I would have qualified for ME/CFS bar the severity requirement and that would include a symptom that would fit the definition of PEM, although I am pretty sure it was distinct from what members here have.
I don't think there will be a significant number with MS. Most MS, even at the first episode, has symptoms and signs that set it apart. Also, I don't think MS follows closely on the heels of IM much - we just have data indicating that MS is more or less always preceded at some time by EBV infection.
I don't think there will be a significant number with MS. Most MS, even at the first episode, has symptoms and signs that set it apart. Also, I don't think MS follows closely on the heels of IM much - we just have data indicating that MS is more or less always preceded at some time by EBV infection.
If I remember my own thoughts correctly, the comment about MS and depression was simply related to Fukuda possibly picking up health issues that might not even be related to post-viral fatigue but to other health problems (be it MS, depression, Hashimoto's, post viral thyroiditis or whatever, I might have singled out depression and MS because there were studies with Fukuda criteria in those conditions) or maybe not even too many problems at all (if I'm reading Simons comments correctly some seem quite healthy), I guess around the 40% of people @Simon is referring to.
I think what you say seems reasonable @Simon M . I see you've beatifully plotted the different scores at different time points. Is there something similar for how many people are in the S-ME/CFS and ME/CFS group at the different times? (Time point 1 might be particularly interesting as we wouldn't expect high rates here, if genuine ME/CFS is supposed to be detected).
How long did they wait to allow time 2, the IM infection to happen (just to understand how feasible this is in general)?
The group is selected based on those meeting the category at 6 months, e.g. S-ME/CFS at 6 months. The scores at baseline and IM (the single measurement point within 6 weeks of symptom onset) are the scores at those timepoints for those that end up in the 6-month category. So things works backwards from the selection at 6 months.
This site uses cookies to help personalise content, tailor your experience and to keep you logged in if you register.
By continuing to use this site, you are consenting to our use of cookies.