I've set this out several times before but I am going to set it out just once more:
The WHO's editorial policy is
not to permit new eponymous names to be used as
Concept Title terms (these are the terms to which the code is assigned, under which may sit a number of Synonyms terms and Index terms,
which may or may not be coded to the
Concept Title code and
which may or may not be listed in the ICD-11 equivalent of the Tabular List).
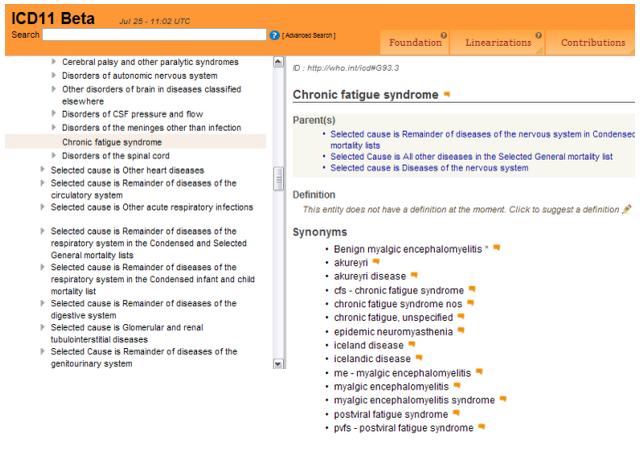
In ICD-11, where there is alternative medical terminology, the medical term is the designated
Concept Title and any eponymous terms are listed under
Synonyms.
WHO ICD-11 Reference Guide on eponyms and use of acronyms:
Example of convention for acronyms under Synonyms or Index terms:
- PVFS - [postviral fatigue syndrome]
- ME - [myalgic encephalomyelitis]
- CFS - [chronic fatigue syndrome]
There are a number of problems with eponyms - here are a few of them:
1 Translations - ICD is translated into dozens of languages, sometimes using non human translators.
2 Lack of knowledge in other countries of the significance of a proposed eponymous term. What would the name "Ramsay", for example, mean to a clinician or patient in Mongolia?
3 Disputes over who first discovered a disease, disorder or finding.
4 Is the proposed eponymous term inclusive of all patients diagnosed with the disease or do some, for example, have non "Ramsay" described onset?
5 An historical eponym may lack specificity and may have been applied to more than one disease or condition.
6 Classification and terminology systems are electronic systems and rely heavily on search engine databases. For ICD-11, the Alphabetical Index is replaced with an electronic Coding Tool. The Index and for ICD-11, the electronic Coding Tool, are the first point of access for coders.
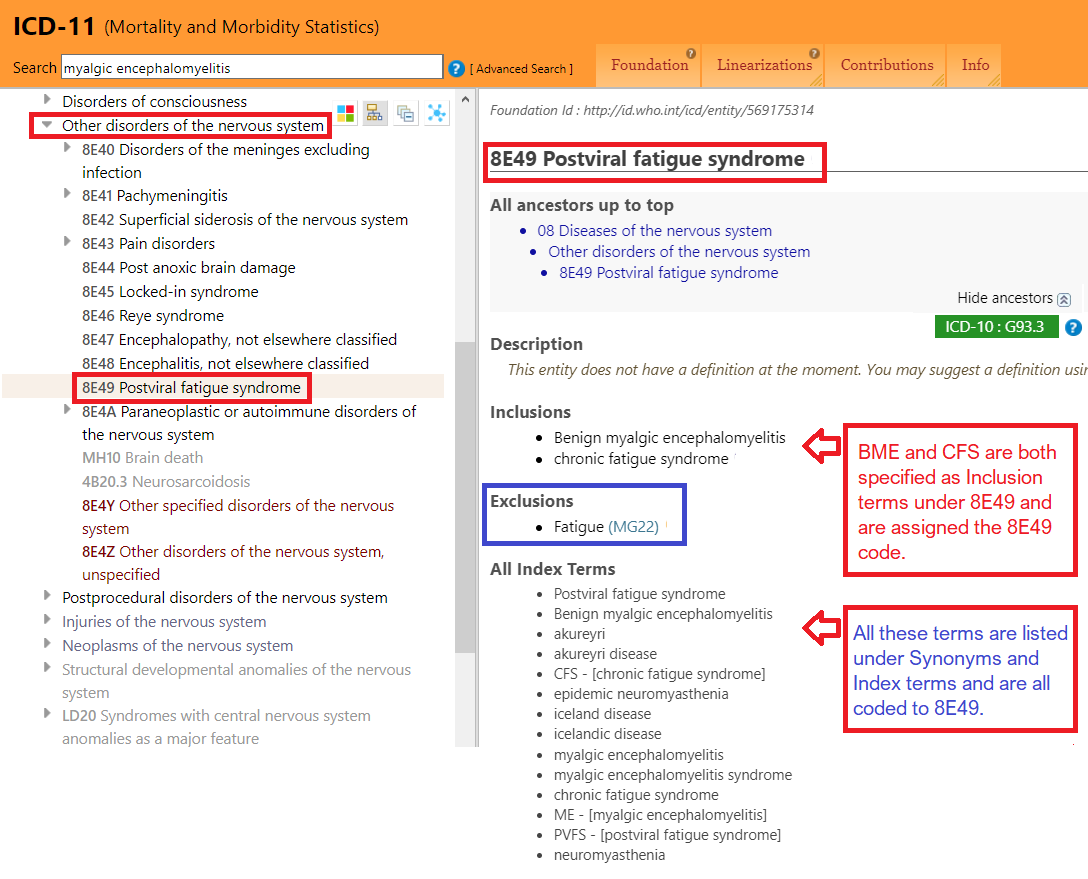
ICD-11 Coding Tool:
https://icd.who.int/devct11/icd11_mms/en/current
As it happens, I can use "Ramsay Hunt Syndrome" as a good example:
The name "Ramsay Hunt" (and sometimes "Ramsay-Hunt") is historically associated with two disorders:
8B88.Y Other specified disorders of facial nerve
Ramsay-Hunt syndrome
Ramsay-Hunt disease or syndrome
and
8A07.Y Other specified movement disorder
Ramsay Hunt cerebellar syndrome
But the Ramsay Hunt and Ramsay-Hunt terms are listed under Synonyms or listed only in the Foundation Component, as opposed to being included in the
ICD-11 Mortality and Morbidity Statistics Linearization (the equivalent of the ICD Tabular List, where the coded-for terms are).
The ICD-11
Preferred term for one of these disorders is:
https://icd.who.int/dev11/f/en#http://id.who.int/icd/entity/305361524
Geniculate ganglionitis
with
- Ramsay-Hunt syndrome
- Ramsay-Hunt disease or syndrome
- Hunt neuralgia
under Synonyms terms.
--------------------------------------------------------------------
SNOMED CT terminology system:
In
SNOMED CT terminology system, a search on "Ramsay" will return the following choices. SNOMED CT uses
"Ramsay Hunt Syndrome 1" and
"Ramsay Hunt Syndrome 2" in the search engine database, to differentiate between two disorders historically associated with the term, "Ramsay Hunt Syndrome".
There is also a:
Ramsay sedation scale (Concept term and Preferred term is: 281400004 Ramsay sedation scale)
A
Concept term in SNOMED CT is the "Fully Specified Name (FSN)".
In SNOMED CT we have:
Ramsay Hunt Syndrome 1 (Concept term and Preferred term: 41009006 Progressive cerebellar tremor (disorder)
Ramsay Hunt Syndrome 2 (Concept term and Preferred term: 21954000 Herpes zoster auricularis (disorder)
Ramsay Hunt Syndrome - ataxia (Concept term and Preferred term: 192871008 Early onset cerebellar ataxia with myoclonus (disorder)
Ramsay Hunt Syndrome - auricula (Concept term and Preferred term: 21954000 Herpes zoster auricularis (disorder)
--------------------------------------------------------------------
To take "Lou Gehrig disease" as an example of a disease that attracted a lot of public attention:
(In some countries the term motor neuron disease is used synonymously with amyotrophic lateral sclerosis.)
In ICD-11 it is listed as:
8B60 Motor neuron disease
Lou Gehrig disease is listed under Synonyms terms along with a number of alternative terms.
For SNOMED CT, the Concept term and Preferred term is:
86044005 Amyotrophic lateral sclerosis
again, with Lou Gehrig's disease under the Synonyms list:
en Amyotrophic lateral sclerosis
en Amyotrophic lateral sclerosis (disorder)
en Bulbar motor neuron disease
en ALS - Amyotrophic lateral sclerosis
en Lou Gehrig's disease
-------------------------------------------
Note that for ICD-11, where an eponymous name is listed under Synonyms, it should drop any genitive "s".
So ICD-11 lists "Lou Gehrig disease" under Synonyms terms - not "Lou Gehrig's disease".