ME/CFS Science Blog
Senior Member (Voting Rights)
Sorry for the long delay. Here’s a short summary of the Belgian assessment report.
Part I
The first 60 pages give an overview of international developments and there are a lot of good things mentioned. The report says ME/CFS is a serious condition (can be more disabling than MS), recognized by the WHO as a disorder of the CNS and nowhere to be found in the DSM 5. It acknowledges the trend towards biomedical research in the US, Australia and Norway. It explains why the Oxford criteria are too broad and no longer accepted in ME/CFS research. And it explains that GET should no longer be advised to patients with ME/CFS as this can be harmful. Instead exercise within personal limits is proposed.
There’s also a section on PACE-gate where most of the problems with the PACE-trial are explained, even though they call it an “emotional and dogmatic discussion” (with lots of cartesian dualism) What’s interesting is that the authors think the PACE-trial has embarrassed the BPS model and research into CBT. The say that:
They then go on to defend the BPS model and indicate it hasn’t been used in its normal meaning in ME/CFS.
One of these models, the Dutch model of CBT – is explicitly criticized in the report.
They also criticize the idea that CBT can cure ME/CFS and say this assumption has never been used in their ME/CFS centre. As an alternative they propose the stress adaptation model as this model is more in agreement with biomedical findings. It assumes that the stress response in ME/CFS stress is defect and that this can explain immune and endocrine abnormalities. In this stress adapation model psychosocial factors are not assumed to be driving symptoms but seen as merely ‘modulators’. You can learn more about it on the MEpedia page of Boudewijn Van Houdenhove – the former head of the CFS centre at Leuven who has promoted this theory. It places a lot of emphasize on childhood trauma (many reference s to Heim et al.), perfectionism and the idea that overdoing it leads to a “allostatic crash” that cannot easily be restored.
The report acknowledges some biomedical abnormalities in ME/CFS such as elevated cytokines, reduced blood volume and metabolic defects (there’s even reference to the Nakatomi et al. 2014 PET study). But they say that these are not specific to ME/CFS and found in other diseases as well. There hasn’t been a biomarker or pathological finding that is unique to ME/CFS and according to the authors this is partly because ME/CFS is a very heterogeneous condition.
A section also discusses the ICC, of which they are not a fan:
They argue that the last two have not been demonstrated in ME/CFS. The authors seem to prefer the IOM-criteria in diagnosing ME/CFS, even though they acknowledge that these are not intended for research.
PART II
So that was the long introduction, now on to the actual data.
Even though the authors (mostly psychiatrists and psychologists) acknowledge the flaws with GET, they still defend CBT. Although they say it should not aim at full recovery, they call it rehabilitation (with the aim of restoring enough of the patients’ health so they can go back to work). This approach is now being evaluated in the assessment report. Because a government agency (RIZIV/INAMI) was paying for the treatment and diagnostic investigation, it wanted a 4-year assessment report to see how things are going.
The last time such a report was published was in 2006. This is the famous Belgian report that showed that employment decreased and disability payments increased after GET/CBT. Instead of realizing that these treatments are inappropriate for ME/CFS patients, it was argued that some small adjustments would make things ok and bring the results in agreement with those reported in scientific studies.
GET and CBT would no longer be offered in group format (which was the case before 2006) and primary care became integrated in the treatment of ME/CFS. The patient should get an individualized treatment from a trained psychologist (CBT) or physiotherapist (GET) in his neighborhood. The CFS centre is only there to make the diagnosis and coordinate things. Most CFS-centres in Belgium did not agree with this approach (they didn’t think it was realistic or they wanted to treat the patients in their centre themselves). So only one CFS-centre signed up for the agreement: the largest one at Leuven. They focus mostly on CBT.
The data the CFS-centre at Leuven offers in this report is a bit confusing because they do not simply show the results of patients who have been through all the assessments and finished the treatment. Data of patients who are still in treatment are added as well, which makes it hard to compare outcomes from baseline, assessment 1, 2 or at the end of treatment. In the graph I will show below, you often see a large drop in the number of patients who provided the final outcome measurement. These do not all present drop-outs but simply patients who are still in treatment and haven’t reached the final outcome measurement yet.
Despite that, the attrition rate was in fact quite large. 12% of patients to whom the treatment was offered, refused. Another 13% dropped out during treatment. It also seems that CBT treatment was not offered to all patients who’ve received a ME/CFS (Fukuda-criteria) diagnosis at Leuven (see discussion in posts above).
I have tried to summarize the main data in the graph below (SD is the standard deviation, n the number of patients providing data). While there was some improvement in fatigue, the change in physical function is probably not clinically significant. After 15 sessions of CBT, the patients still scores less than 60, which we know from PACE-gate is close to the mean score for patients with Class II congestive heart failure. Scores for depression and positive/negative affect did not show a significant change over time. Other questionnaires did show some improvement but as there was no control group we cannot know if this was due to CBT.

Data about employment are also given, but here they take a different approach and focus only on those who have completed the full treatment (147 patients). The data is a bit messy and they do not give standard deviations or p-values.

It seems that some patients who were not working at baseline, did go into part-time work. But at the same time the number of patient who were working full time halved, as many also switched to part-time work. In all, it seems that there were some minor improvements in work resumption, but we cannot know if this was statistically significant over time. There was also no control group, so any improvement could be due to being diagnosed or receiving medical care in a specialist centre, not necessarily CBT.
In parliament the minister said “work resumption difficulties are an important disease-maintaining factor”. This refers to the following. The doctors at Leuven gave each of their patients a label +, +/- or – indicating how easy it was for the patient to resume work if their health improved. Then they showed that the patients receiving a - at baseline showed less improvements after treatment. Not exactly cutting edge science I would say… In a similar fashion they argue that patients learned to avoid boom and bust cycles, because the (self-reported) differences in activity between a good and a bad day, decreased.
According to the authors of the report, the results are good because most patients indicate their health has improved (76%) or that their activity level increased (66%). They have asked to extend the convention, even though they caution CBT should be tailored to the individual and is not necessarily useful for every ME/CFS patient.
THE END
Part I
The first 60 pages give an overview of international developments and there are a lot of good things mentioned. The report says ME/CFS is a serious condition (can be more disabling than MS), recognized by the WHO as a disorder of the CNS and nowhere to be found in the DSM 5. It acknowledges the trend towards biomedical research in the US, Australia and Norway. It explains why the Oxford criteria are too broad and no longer accepted in ME/CFS research. And it explains that GET should no longer be advised to patients with ME/CFS as this can be harmful. Instead exercise within personal limits is proposed.
There’s also a section on PACE-gate where most of the problems with the PACE-trial are explained, even though they call it an “emotional and dogmatic discussion” (with lots of cartesian dualism) What’s interesting is that the authors think the PACE-trial has embarrassed the BPS model and research into CBT. The say that:
“PACE-gate has unintentionally and unjustifiably done a lot of damage to the credibility of CBT and GET as possible therapeutic options in CFS/ME and especially to the multidisciplinary, biopsychosocial research, diagnosis and treatment in patients with CFS/ME.”
They then go on to defend the BPS model and indicate it hasn’t been used in its normal meaning in ME/CFS.
“In the complex world of CFS/ME there has been a confusion of speech, whereby ‘BPS’ as an umbrella term came to mean a psychogenic/psychosocial etiology and a number of specific models that suggested a psychosocial/behavioural hypothesis of pathology."
One of these models, the Dutch model of CBT – is explicitly criticized in the report.
"The Dutch "deconditioning model" that is used in ME/CFS focuses very much on adjusting cognitions and behaviour and takes too little account of the specific situation of the CFS/ME patient (i.e., it is assumed that the symptoms are maintained by ineffective thoughts such as "I am tired and if I make an effort my fatigue increases, so I will just rest. According to this model this would lead to deconditioning and an increased attentional bias to physical complaints). To rebuild the physical condition there was, among other things, a forced build-up of activity, without taking into account PEM which is central to CFS/ME patients that led to a relapse, unless it was used on patients with a depression or idiopathic fatigue. The Dutch model was never used in Belgium within the framework of the CFS convention.”
They also criticize the idea that CBT can cure ME/CFS and say this assumption has never been used in their ME/CFS centre. As an alternative they propose the stress adaptation model as this model is more in agreement with biomedical findings. It assumes that the stress response in ME/CFS stress is defect and that this can explain immune and endocrine abnormalities. In this stress adapation model psychosocial factors are not assumed to be driving symptoms but seen as merely ‘modulators’. You can learn more about it on the MEpedia page of Boudewijn Van Houdenhove – the former head of the CFS centre at Leuven who has promoted this theory. It places a lot of emphasize on childhood trauma (many reference s to Heim et al.), perfectionism and the idea that overdoing it leads to a “allostatic crash” that cannot easily be restored.
The report acknowledges some biomedical abnormalities in ME/CFS such as elevated cytokines, reduced blood volume and metabolic defects (there’s even reference to the Nakatomi et al. 2014 PET study). But they say that these are not specific to ME/CFS and found in other diseases as well. There hasn’t been a biomarker or pathological finding that is unique to ME/CFS and according to the authors this is partly because ME/CFS is a very heterogeneous condition.
A section also discusses the ICC, of which they are not a fan:
“the presumed common underlying pathogenetic/pathophysiological mechanisms do not justify the proposed categories.”
They argue that the ICC places too much emphasis on an infectious hypothesis. One section is particularly interesting, so I translated it in full:
“It is also important to emphasize that finding a certain degree of central inflammatory parameters, as is the case with ME/CFS, does not always indicate neuroinflammation. The term "Neuroinflammation" is currently reserved when 4 classical characteristics are present: (i) increase in proinflammatory cytokines (ii) microglial activation (iii) infiltration of peripheral leukocytes (iv) secondary neurodegeneration.”
They argue that the last two have not been demonstrated in ME/CFS. The authors seem to prefer the IOM-criteria in diagnosing ME/CFS, even though they acknowledge that these are not intended for research.
PART II
So that was the long introduction, now on to the actual data.
Even though the authors (mostly psychiatrists and psychologists) acknowledge the flaws with GET, they still defend CBT. Although they say it should not aim at full recovery, they call it rehabilitation (with the aim of restoring enough of the patients’ health so they can go back to work). This approach is now being evaluated in the assessment report. Because a government agency (RIZIV/INAMI) was paying for the treatment and diagnostic investigation, it wanted a 4-year assessment report to see how things are going.
The last time such a report was published was in 2006. This is the famous Belgian report that showed that employment decreased and disability payments increased after GET/CBT. Instead of realizing that these treatments are inappropriate for ME/CFS patients, it was argued that some small adjustments would make things ok and bring the results in agreement with those reported in scientific studies.
GET and CBT would no longer be offered in group format (which was the case before 2006) and primary care became integrated in the treatment of ME/CFS. The patient should get an individualized treatment from a trained psychologist (CBT) or physiotherapist (GET) in his neighborhood. The CFS centre is only there to make the diagnosis and coordinate things. Most CFS-centres in Belgium did not agree with this approach (they didn’t think it was realistic or they wanted to treat the patients in their centre themselves). So only one CFS-centre signed up for the agreement: the largest one at Leuven. They focus mostly on CBT.
The data the CFS-centre at Leuven offers in this report is a bit confusing because they do not simply show the results of patients who have been through all the assessments and finished the treatment. Data of patients who are still in treatment are added as well, which makes it hard to compare outcomes from baseline, assessment 1, 2 or at the end of treatment. In the graph I will show below, you often see a large drop in the number of patients who provided the final outcome measurement. These do not all present drop-outs but simply patients who are still in treatment and haven’t reached the final outcome measurement yet.
Despite that, the attrition rate was in fact quite large. 12% of patients to whom the treatment was offered, refused. Another 13% dropped out during treatment. It also seems that CBT treatment was not offered to all patients who’ve received a ME/CFS (Fukuda-criteria) diagnosis at Leuven (see discussion in posts above).
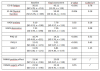
I have tried to summarize the main data in the graph below (SD is the standard deviation, n the number of patients providing data). While there was some improvement in fatigue, the change in physical function is probably not clinically significant. After 15 sessions of CBT, the patients still scores less than 60, which we know from PACE-gate is close to the mean score for patients with Class II congestive heart failure. Scores for depression and positive/negative affect did not show a significant change over time. Other questionnaires did show some improvement but as there was no control group we cannot know if this was due to CBT.
Data about employment are also given, but here they take a different approach and focus only on those who have completed the full treatment (147 patients). The data is a bit messy and they do not give standard deviations or p-values.
It seems that some patients who were not working at baseline, did go into part-time work. But at the same time the number of patient who were working full time halved, as many also switched to part-time work. In all, it seems that there were some minor improvements in work resumption, but we cannot know if this was statistically significant over time. There was also no control group, so any improvement could be due to being diagnosed or receiving medical care in a specialist centre, not necessarily CBT.
In parliament the minister said “work resumption difficulties are an important disease-maintaining factor”. This refers to the following. The doctors at Leuven gave each of their patients a label +, +/- or – indicating how easy it was for the patient to resume work if their health improved. Then they showed that the patients receiving a - at baseline showed less improvements after treatment. Not exactly cutting edge science I would say… In a similar fashion they argue that patients learned to avoid boom and bust cycles, because the (self-reported) differences in activity between a good and a bad day, decreased.
According to the authors of the report, the results are good because most patients indicate their health has improved (76%) or that their activity level increased (66%). They have asked to extend the convention, even though they caution CBT should be tailored to the individual and is not necessarily useful for every ME/CFS patient.
THE END