2024 release of ICD-10-CM:
The files for the
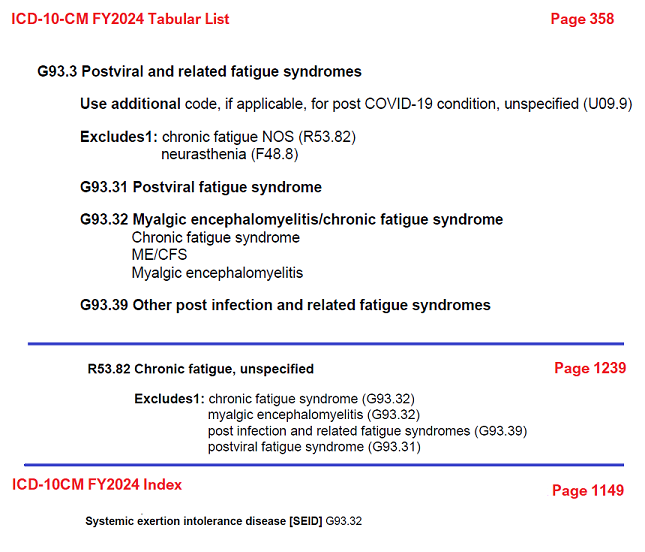
FY2024 ICD-10-CM codes have been posted on the CDC's website.
These codes are to be used from October 1, 2023 through September 30, 2024 and replace the FY2023 – April 1, release.
The FY2024 Guideline document, Addenda, Tabular List, Index etc can be downloaded as standalone PDFs, or in some cases, within Zip files from:
https://cdc.gov/nchs/icd/Comprehensive-Listing-of-ICD-10-CM-Files.htm
For ease of access, PDF copies of the Tabular List and Index can be downloaded from my website:
FY2024 Tabular List [7MB]:
https://dxrevisionwatch.files.wordpress.com/2023/07/icd10cm-tabular-2024.pdf
FY2024 Index [9MB]:
https://dxrevisionwatch.files.wordpress.com/2023/07/icd10cm-index-2024.pdf
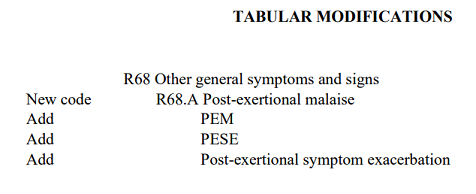
Update on status of March 2023 proposal for a unique code for PEM/PESE to be added to Symptoms, signs chapter:
There has been no approval and implementation of the proposal for a unique code for PEM/PESE to be added to the Symptoms, signs chapter of ICD-10-CM for the FY2024 release. (It had been clarified by CDC's Traci Ramirez, in March, that the proposal submitted by the Patient-Led Research Collaboration was not being considered for fast track implementation.)
According to the Patient-Led Research Collaborative, the proposal to add a code for PEM/PESE is going to be revisited at the September '23 meeting
"with minor changes in response to feedback".
P-LRC has said they do not yet have final details on what the changes presented at the next meeting will be. It is also unclear to me at this point whether the revised proposals are going to be presented by CDC, or by both CDC and on behalf of the P-LRC.
The next virtual meeting of the ICD-10-CM C&M Committee is scheduled for September 12 – 13.
The Tentative Agenda is usually released a month or so before the meeting via a Notice in the Federal Register and is also posted on the CDC's ICD-10-CM C&M
Upcoming Meetings page. The Tentative Agenda only lists some of the topics for consideration at the next meeting and no rationales or setting out of proposed coding structures.
The full agenda (Topic Packet) which should include the full list of topics for discussion and the proposal rationales is usually released a day or two before meeting Day 1. So this may not be publicly available until Monday, 11 September.
It's unclear at this point whether P-LRC will be informed of the proposed revisions
prior to the meeting and if so, whether they will
publicly circulate what they know in good time, in order that advocacy groups, patients and their carers might review these proposed revisions prior to the meeting taking place.