PDF version: https://dxrevisionwatch.files.wordpress.com/2020/02/new-proposal-for-icd-11-remove-benign-1.pdf
or Bitly Custom Link:
http://bit.ly/BenignICD11
ICD-11 Orange Maintenance Platform: Proposal Mechanism
(Registration with the platform is required to access Proposals)
https://icd.who.int/dev11/proposals...lGroupId=d9877203-d434-42b2-9f5f-cd649d259aec
2020-Feb-09 - 17:49 #298U Originator: Suzy Chapman
Edit to text and to insert additional reference. Proposal now date stamped:
2020-Feb-14 - 09:26 #298U
Complex Hierarchical Changes Proposal
Proposal Status: Submitted
Postviral fatigue syndrome
Detailed Explanation of the Proposal
Declarations: The author of this submission has no affiliations and no conflicts of interest to declare.
The following changes to the specified Inclusions under 8E49 Postviral fatigue syndrome are proposed:
Remove inclusion term: Benign myalgic encephalomyelitis
Add inclusion term: Myalgic encephalomyelitis
It is recommended to retain the entity "Benign myalgic encephalomyelitis" under the Synonyms/Index Terms list for continuity with ICD-10 and the various national modifications of ICD-10.
There is an
exclusion for "Benign myalgic encephalomyelitis (8E49)" under 6C20 Bodily distress disorder (Foundation Id:
http://id.who.int/icd/entity/767044268)
There is an
exclusion for "(Benign) myalgic encephalomyelitis (8E49)" under MG22 Fatigue (Foundation Id:
http://id.who.int/icd/entity/1109546957)
Please revise both of these exclusions under 6C20 and MG22 to Myalgic encephalomyelitis (8E49).
Rationale
The Rationale for this proposal is being appended to the Detailed Explanation for improved accessibility for a stakeholder patient group, some of whom may experience cognitive impairment and visual problems when viewing unformatted plain texts on computers and other devices.
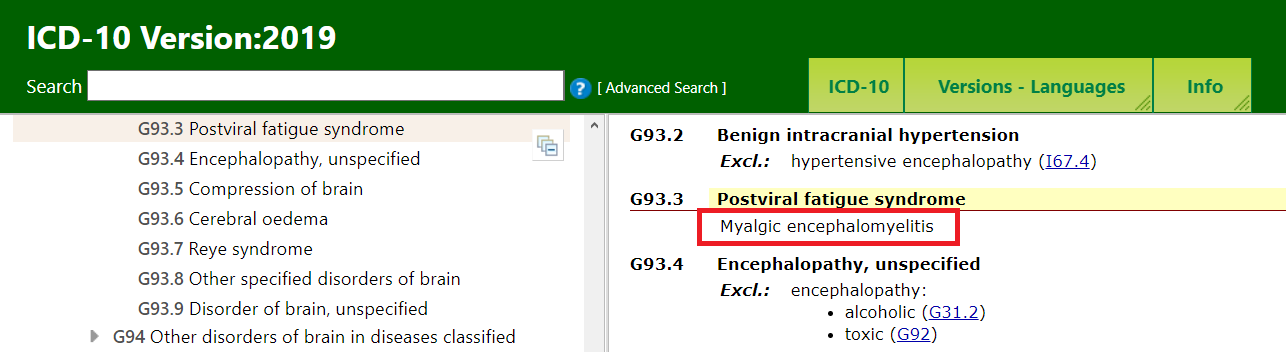
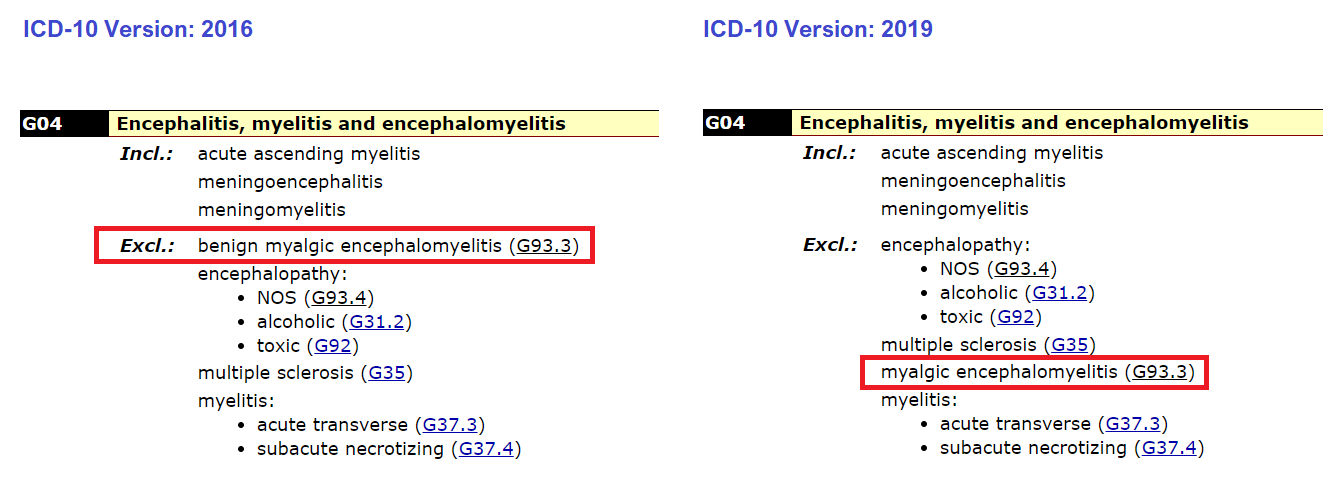
1 Consistency with ICD-10: A new release of ICD-10 (ICD-10 Version: 2019) has recently been published on the ICD-10 Browser platform [1]. Under the G93.3 Postviral fatigue syndrome concept title, the inclusion term "Benign myalgic encephalomyelitis" has been revised to "Myalgic encephalomyelitis". This decision establishes a precedent for ICD-11. For consistency and continuity with ICD-10, the prefix "Benign" should also be deprecated for the 8E49 specified inclusion term. (It is recommended to retain the entity "Benign myalgic encephalomyelitis" under the Synonyms/Index Terms list for backward compatibility and comparability over time.)
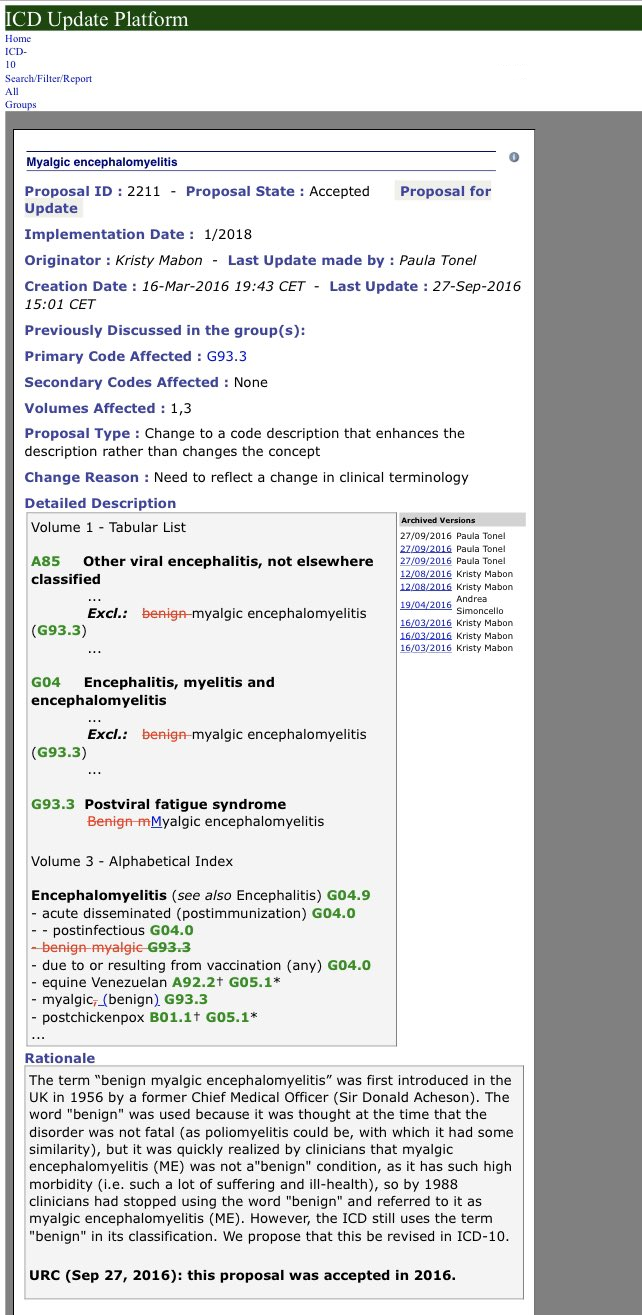
It has come to my attention that a proposal for revision of "Benign myalgic encephalomyelitis" to "Myalgic encephalomyelitis" for ICD-10 was submitted to the URC (Update and Revision Committee) on March 16, 2016 by Ms Kristy Mabon, a Classification Specialist at Canadian Institute for Health.
Proposal ID: 2211: Accepted
Screenshot:
http://bit.ly/2SCM3cA
The proposal is marked:
URC (Sept 27, 2016): this proposal was accepted in 2016. Implementation date: 1/2018.
Since a proposal for deletion of the prefix "Benign" had already been accepted by the URC in 2016, for implementation in ICD-10 from 1/2018, there appears to be no basis for the same proposal submitted by Chapman and Dimmock (March 31, 2017 as part of a multi-part submission for ICD-11) being rejected outright in March 2019 (Team3 WHO 2019-Mar-04 - 22:58 UTC). Several requests for the rationale for the decision to reject this proposal have met with no response [14].
As URC proposal ID: 2211 has now been incorporated into ICD-10 Version: 2019, this further supports its migration to ICD-11.
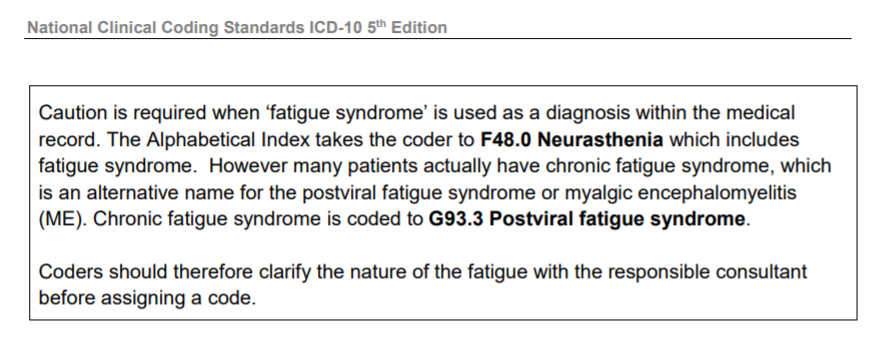
2 Deprecation of the prefix "Benign" by international health agencies: NHS England, NHS Digital National Clinical Coding Standards, NICE (National Institute for Health and Care Excellence), CDC (Centers for Disease Control and Prevention), U.S. National Academy of Medicine, DIMDI (Deutsche Institut für Medizinische Dokumentation und Information) and the Australian Consortium for Classification Development all use the term "Myalgic encephalomyelitis" in preference to "Benign myalgic encephalomyelitis" [2-5]. The German ICD-10-GM and Australian ICD-10-AM have already deprecated the "Benign" prefix in the Tabular Lists of their national modifications [6-7].
3 Disease burden and impact on functional status: The disease is associated with substantial impairment in functioning. Patients have been found to be more functionally impaired than those with other disabling illnesses, including type 2 diabetes mellitus, congestive heart failure, multiple sclerosis and end-stage renal disease (Jason and Richman, 2008). Papers discussing quality of life and impact on functional status [8-11].
The 2015 Report of the U.S. National Academy of Medicine concluded that the disease is a
"serious, chronic, complex, and multisystem disease" that causes neurological, cognitive, immunological, autonomic, and energy metabolism impairment. The Report also noted that the disease can result in prolonged and significant disability with impairment in ability to engage in educational, occupational, social and personal activities; that there is a considerable economic burden associated with these conditions, with many patients unable to continue in employment; that 25% of patients are bed- or house-bound during their illness and that severely affected patients will require very high levels of personal care and assistance [5].
Some severely affected patients may develop weakness of the muscles of the mouth and throat resulting in difficulty speaking and swallowing food, fluids and medications. Some cases necessitate administration of fluids and nutrition via abdominal PEG tubes (percutaneous endoscopic gastrostomy).
4 Mortality: For at least the last 17 years, researchers have published studies reporting an increased risk of death due to cancer, cardiac disease, and suicide. On July 11, 2009, autopsy evidence was presented at a Royal Society of Medicine meeting by Dr Abhijit Chaudhuri, Essex Centre for Neurosciences, where slides of inflammation of dorsal root ganglia in three patients with myalgic encephalomyelitis were discussed [12]. A disease specific post-mortem brain and tissue bank for the study of myalgic encephalomyelitis and chronic fatigue syndrome was proposed for the UK [13].
5 Deaths registered in England and Wales, 2001 to 2016, Freedom of Information Request: Office of National Statistics, Information request release date: 18 May 2018, Reference number: 008461. Mentions of postviral fatigue syndrome (benign myalgic encephalomyelitis), in deaths registered in England and Wales, 2001 to 2016:
https://www.ons.gov.uk/peoplepopula...isdeathsregisteredinenglandandwales2001to2016
Summary of FOI request: This table presents the number of deaths that mentioned postviral fatigue syndrome (benign myalgic encephalomyelitis) on the death certificate, either as the underlying cause of death or as a contributory factor. Figures are based on deaths registered in England and Wales between 2001 and 2016:
https://www.ons.gov.uk/file?uri=/pe...redinenglandandwales2001to2016/finaltable.xls
6 Stakeholder support for deprecation of the "Benign" prefix: In a proposal submitted by Chapman & Dimmock (March 27, 2017; minor edit March 31, 2017), the authors had recommended, inter alia, to delete the prefix "Benign" from the "Benign myalgic encephalomyelitis" inclusion term and replace the entity with "Myalgic encephalomyelitis".
The authors argued that given the high burden of morbidity associated with the disease and recorded mortality, there was no justification for retaining the designation "Benign" for ICD-11. Around 40 international patient organisations submitted responses in support of deprecation of the "Benign" prefix [14].
In sum: it fails to reflect the high burden of morbidity or acknowledge recorded mortalities; it does a disservice to patients and to families caring for adults, children and young people and to the families of those who have died as result of the disease, some whilst still in their 20s and 30s.
References
1 ICD-10 Version: 2019, Accessed February 09, 2020:
https://icd.who.int/browse10/2019/en#/G93.3
2 NHS Digital National Clinical Coding Standards ICD-10 5th Edition (2019) p84:
https://hscic.kahootz.com/gf2.ti/f/...oding_Standards_ICD10_reference_book_2019.pdf
3 NICE CG53: Chronic fatigue syndrome/myalgic encephalomyelitis (or encephalopathy): diagnosis and management Clinical guideline [CG53] Published date: August 2007:
https://www.nice.org.uk/guidance/cg53/chapter/1-guidance
Revision of NICE CG53: Myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome: diagnosis and management In development [GID-NG10091]:
https://www.nice.org.uk/guidance/indevelopment/gid-ng10091/
4 CDC (Centers for Disease Control and Prevention):
https://www.cdc.gov/me-cfs/index.html
5 National Academy of Medicine:
http://www.nationalacademies.org/hmd/Reports/2015/ME-CFS.aspx
6 ICD-10-GM, DIMDI:
https://www.dimdi.de/static/de/klas...m/kode-suche/htmlgm2019/block-g90-g99.htm#G93
7 ICD-10-AM, Australian Consortium for Classification Development:
https://www.ihpa.gov.au/what-we-do/icd-10-am-achi-acs-current-edition
8 Falk Hvidberg M, Brinth LS, Olesen AV, Petersen KD, Ehlers L (2015). The Health-Related Quality of Life for Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS):
https://journals.plos.org/plosone/article?id=10.1371/journal.pone.0132421
9 Nacul LC, Lacerda EM, Campion P, Pheby D, de L Drachler M, Leite JC et al. The functional status and well being of people with myalgic encephalomyelitis/chronic fatigue syndrome and their carers. BMC Public Health 2011 11:402:
https://bmcpublichealth.biomedcentral.com/articles/10.1186/1471-2458-11-402
10 Eliana M. Lacerda Kingdon, C.C., Bowman, E.W., Curran, H. et al. Functional Status and Well-Being in People with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Compared with People with Multiple Sclerosis and Healthy Controls. PharmacoEconomics Open (2018) 2: 381:
https://link.springer.com/article/10.1007/s41669-018-0071-6
11 Dimmock ME, Mirin AA, Jason LA (2016). Estimating the disease burden of ME/CFS in the United States and its relation to research funding. J Med Therap 1: doi:10.15761/JMT.1000102:
https://oatext.com/Estimating-the-d...ates-and-its-relation-to-research-funding.php
12 O’Donovan D, Harrower T, Cader S, Findley L, Shepherd C, Chaudhuri A. Pathology of Chronic Fatigue Syndrome: Pilot Study of four autopsy cases. International Science Symposium 3-4 – Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) Queensland, Australia: Population Health and Neuroimmunology Unit, Bond University; 2010.
13 Nacul L, O’Donovan DG, Lacerda EM, et al. Considerations in establishing a post-mortem brain and tissue bank for the study of myalgic encephalomyelitis/chronic fatigue syndrome: a proposed protocol. BMC Research Notes. 2014;7:370:
http://bmcresnotes.biomedcentral.com/articles/10.1186/1756-0500-7-370
14 Proposal Mechanism, Chapman & Dimmock (March 31, 2017):
https://icd.who.int/dev11/proposals...lGroupId=4b26ab6a-393f-4a39-9051-4ac1d4b1a55a
--------------------------------------------------------------------------------
Edited to include additional text and insertion of an additional reference.
--------------------------------------------------------------------------------
NB: The latest edition of the
National Clinical Coding Standards ICD-10 5th Edition Reference Book 2020 (for implementation April 1st 2020) in reference 2 is now available for download from the NHS Digital Delen Resource pages:
https://hscic.kahootz.com/connect.ti/t_c_home/view?objectId=16878800
https://hscic.kahootz.com/gf2.ti/f/762498/63579813.1/PDF/-/NCCSICD20206.pdf
As with earlier versions of this ICD-10 Coding Standards, it includes the following guidance: