Inara
Senior Member (Voting Rights)
This thread refers to @Dx Revision Watch's allusion to their proposal to WHO to change the ME caption in ICD-11, see https://dxrevisionwatch.com/2017/04...cd-10-g93-3-legacy-terms-for-icd-11-part-one/ and https://dxrevisionwatch.com/2017/04...cd-10-g93-3-legacy-terms-for-icd-11-part-two/
First, many thanks to you for pointing to this process, I didn't know of it.
I understood your aims are the following (citation from Part Two):
Just a side question: Science literature gives several clues that ME is somehow linked to an immune disfunction/deficiency/pathology - isn't that important for categorizing in ICD? What counts is the major system affected (like in MS, e.g.)?
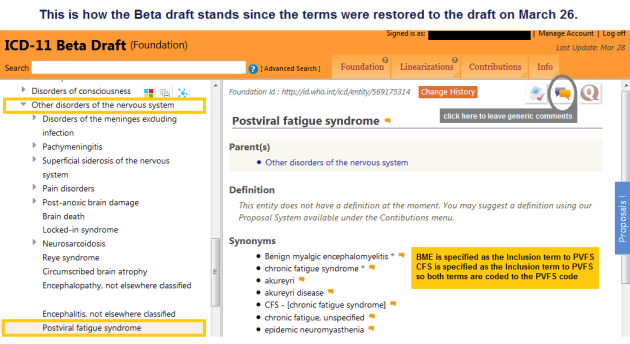
In your proposal, PVFS shall sit under ME as a synonym.
A synonym is a different term to an exististing term for a common object, i.e. behind each synonym are common characteristics of this one object. Each exististing term can be used interchangeably without changing the meaning.
So, if I read in ICD-10 "PVFS" and then "synonyms", I understand that I can use each expression interchangeably, while always the same object is meant. This doesn't change if PVFS sits under ME, these are still synonyms.
However, I guess WHO doesn't mean it that way, does it?
Here my questions:
I'd be happy if my questions found some answers!")
First, many thanks to you for pointing to this process, I didn't know of it.
I understood your aims are the following (citation from Part Two):
- that the terms should be retained in the neurological chapter (Chapter 08: Diseases of the nervous system);
- that the terms should be retained under the parent class: Other disorders of the nervous system;
- that ME and CFS should each be assigned separate codes;
- that PVFS is not an appropriate title term for ME to sit under (not all cases of ME are preceded by a virus).
Just a side question: Science literature gives several clues that ME is somehow linked to an immune disfunction/deficiency/pathology - isn't that important for categorizing in ICD? What counts is the major system affected (like in MS, e.g.)?
In your proposal, PVFS shall sit under ME as a synonym.
A synonym is a different term to an exististing term for a common object, i.e. behind each synonym are common characteristics of this one object. Each exististing term can be used interchangeably without changing the meaning.
So, if I read in ICD-10 "PVFS" and then "synonyms", I understand that I can use each expression interchangeably, while always the same object is meant. This doesn't change if PVFS sits under ME, these are still synonyms.
However, I guess WHO doesn't mean it that way, does it?
Here my questions:
- If not every case of ME follows a viral infection, wouldn't it be correct to remove it completely? Or to have an extra code for PVFS?
- You want an extra code for CFS and ME. This means you assume both medical diseases are disjunct (with possibly common symptoms). Why is that? What are the symptoms that make each disease unique and disjunct?
- Is it reasonable to propose an ICD change of categorization when the underlying processes and pathologies in ME aren't still completely understood and subgroups aren't clearly identified? It's not even clear today if any of the names "ME, CFS, CFIDS, SEID" and so on are good descriptions of the disease.
- In UK, preferably ME is used, in USA ME/CFS (?), and in Germany (unfortunately) CFS. At least here, nearly every doctor doesn't even know there is an ICD code G93.3 - not even neurologists. I am pretty sure no one here knows or will know the difference between "CFS" and ME (if one exists, see above). Some have heard of the "psychological illness CFS" (which has no ICD code). So my concern is that at least for Germans it will be made even harder to escape the psycho stigma.
- Some say "CFS" is no disease at all, see e.g. The Nightingale foundation. They say, behind "CFS" must be other medical or psychological illnesses.
- In my opinion, "CFS" s a brutal euphemism which is laughed about. People who hear "chronic fatigue" in fact hear "chronically tired" (not many know there is indeed a difference, including doctors) which is ridiculous. The reactions are accordingly. You are instantly put into the psycho corner, for one. "Myalgic encephalomyelitis" may not be correct - since not all affected seem to have muscle pain and/or brain inflammation (but how do they know exactly?!) - but the ICC experts have a different opinion. So at this point, I think it's more important to acknowledge that if people hear "myalgic encephalomyelitis" they look at you and say: "That sounds terrible! What is that?" which hits the reality better than "poor you, soooo tired, yes? Just need to find your fulfilling job or another partner!"

I'd be happy if my questions found some answers!