You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Long Covid in the media and social media 2023
- Thread starter rvallee
- Start date
- Status
- Not open for further replies.
Sly Saint
Senior Member (Voting Rights)
Why viral reservoirs are a prime suspect for long COVID sleuths
https://www.npr.org/sections/health...rs-are-a-prime-suspect-for-long-covid-sleuths
deja vu?
Brent Palmer's first inkling about long COVID started in the early days of the pandemic, before the term "long COVID" even existed.
Some of his friends had caught the virus while on a ski trip and returned home to Colorado with the mysterious, new illness. It was a frightening time — and an irresistible opportunity for Palmer, who studies the immune response to infectious diseases like HIV.
In particular, he was keen to see how their T cells, part of the immune system's arsenal for fighting infections, were handling the novel infection. So he started taking samples of their blood. And there was one subject in particular who intrigued him. She was still dealing with heart palpitations, chest pains and trouble breathing more than six weeks after her acute illness.
In the lab, Palmer noticed that she still had a very high percentage of these T cells directed at the virus compared to her husband who'd also fallen ill, but didn't have lingering symptoms. "They had very different responses," says Palmer, an associate professor of medicine at the University of Colorado.
Typically, T cells aimed at the virus reach very high levels during the acute infection and over time they drop off, but Palmer noticed that wasn't the case as he began studying more patients with these persistent symptoms.
"These individuals had frequencies that were 100-fold higher in some cases than the individuals that didn't have any persistent symptoms," he says.
In fact, Palmer says it was like their body was still fighting the virus. It led him to questions: "Despite the fact that they test negative in a nasal swab, is the virus still persisting in the lungs? Is it persisting in some other organ?"
Other scientists trying to uncover the roots of long COVID have asked some version of that same question for the last few years now. This theory of "viral persistence" posits that some people never fully eliminate the infection, that viral reservoirs are subsisting in the body and possibly triggering the symptoms of long COVID.
While a direct link isn't yet proven, this line of research has gained momentum as more evidence has emerged indicating that some people seem to harbor "viral reservoirs'' after their initial illness has passed. It's far from the only explanation under consideration, but some scientists see it as one of the most promising.
https://www.npr.org/sections/health...rs-are-a-prime-suspect-for-long-covid-sleuths
deja vu?
Shadrach Loom
Senior Member (Voting Rights)
Nice Grauniad article about cosmologist and pwLC Catherine Heymans, who is challenging the standard cosmological model with novel accounts of dark matter and dark energy. Prior to covid, Heymans suffered from EBV and glandular fever.
https://www.theguardian.com/science...-universe-the-cosmologist-battling-long-covid
https://www.theguardian.com/science...-universe-the-cosmologist-battling-long-covid
https://www.theguardian.com/science...-universe-the-cosmologist-battling-long-covid
https://www.theguardian.com/science...-universe-the-cosmologist-battling-long-covid
Same old same old. So it's looking more and more like the most likely explanation is the one that will see the fiercest defiance. Medicine has huge hang-ups about any combination of chronic and an infectious pathogen, it's considered a truism that this is not a thing, they can't handle this truth. Other than in exceptions, I guess. It's all so arbitrary. I don't see it all that often, but it's still commonly derided as the "new" chronic Lyme, the very concept isn't just taboo, it's basically toxic poison.Why viral reservoirs are a prime suspect for long COVID sleuths
https://www.npr.org/sections/health...rs-are-a-prime-suspect-for-long-covid-sleuths
deja vu?
It's actually a legitimate question whether they can get over it. It's a very realistic scenario that this ends up being the explanation, but is held off for years out of sheer defiance and inability to process decades of mockery and rejection of what may be one of the most important ideas in all of medicine.
Because it's really not about what's true, it's about what's accepted as true. Normally with professionals you can avoid this problem, but medicine is neck-deep in this nightmare trap. Aside from most basic biology, medical knowledge is largely a social construct, lacking mathematical and experimental proof to end controversy. And it's not as if experience means anything here, this is one profession that can be wrong about something for centuries and never notice anything. They're even still at it.
Kalliope
Senior Member (Voting Rights)
JAMA How Primary Care Physicians Can Recognise and Treat Long COVID (includes interview with among others Lucinda Bateman)
Quote:
Experts interviewed for this story offered some basic guidance for primary care physicians:
Quote:
Experts interviewed for this story offered some basic guidance for primary care physicians:
- Believe the patient. “Say it out loud. They need to hear it,” Palacio said of patients with long COVID symptoms, who are often not believed. If their physician says, “‘I believe you, and I will work with you to try to make you better even though I know very little about this,’ stress levels go down.”
- Go beyond symptoms. Physicians are accustomed to checking off symptoms, but it’s also important to ask, “’How often do these occur?’ and ‘How do they affect your ability to carry out normal daily activities?’” Bateman said. “When you can’t perform physically and cognitively, it starts to really be disabling.”
- Address fatigue. “If patients stop overexerting themselves, they start to feel better. It’s as simple as that,” Brode said. Physicians should discuss with patients “what they can honestly do in their daily activities.”
- Look to familiar conditions. According to the CDC, long COVID can share symptoms with ME/CFS, fibromyalgia, posttreatment Lyme disease syndrome, dysautonomia, and mast cell activation syndrome. Approaches to managing these conditions can help some patients with long COVID. For example, POTS can be alleviated with fluids, compression garments, and graded horizontal exercise.
Mij
Senior Member (Voting Rights)
That's not an admission of defeat, just that the first LC treatment won't be a cure. Never is the initial version of a technology perfect and medicine is no exception. Apparently they also asked what "toxicities" patients would be able to tolerate.
I didn't interpret this as an admission of defeat. I just thought the questioning was odd, "asking patients to select which symptoms they'd want treated the most" and which "ideal treatment". Like, where are we going this?
We share a lot of symptoms with other illnesses. Some pts don't have many or any symptoms except for OI and PEM. A biomarker for PEM would be great to start.
Actually, this annoys me a lot. Angers me, even.Believe the patient. “Say it out loud. They need to hear it,”
Because to be honest here:
It literally does the opposite, because I know they're lying. And I see nothing happening. It has nothing to do with stress, the only reason people go see professionals is because they expect them to do professional-grade work. They really should think less often about stress, they don't really know what to do with the concept anyway. But very little destroys the credibility of professionals than lying on the job. Stop treating people like freaking children, it's annoying and leads to worse outcomes anyway.If their physician says, “‘I believe you, and I will work with you to try to make you better even though I know very little about this,’ stress levels go down.”
I don't want to hear it. I want MDs to act on it. The whole "hearing it" is only meaningful in the sense that it's believed to lead to action. It's like being trapped down a cave with no hope of getting out and hearing someone say "Don't worry, I'll do everything I can to get you out". It only matters if they actually act on it. That would usually involve getting expert help from rescue professionals with equipment and training. If they're only saying it, then walking away, it doesn't count. This is the same exact same here.
Hearing it doesn't mean squat. It's not what they say, it's what they do. And frankly, hearing it from someone who is actually not going to act on it, whether as a choice or because of a system that blocks those efforts, is far worse. Because it's lying. Lying really needs to be banned from healthcare. If the system is blocking those efforts, again we don't need to hear it, we need people to act on it.
Especially as it's a core principle of psychosomatic ideology to say it without meaning it, in fact with the express intent of gaining the patient's confidence by blatantly lying to them. Which really shows how incredibly confused they are about what trust means, or even the nature of their job.
Robert 1973
Senior Member (Voting Rights)
Ritchie’s inews article can be read without paywall here.
Ritchie’s tentative reference to PACE in a Spectator article is discussed here: https://www.s4me.info/threads/stuar...cles-on-science-fraud-and-open-science.21166/
Ritchie
Is he prominent in some way? He looks pretty young for the image.
Robert 1973
Senior Member (Voting Rights)
I don’t think he’s particularly prominent at the moment. He came to my attention when he wrote his book “Science Fictions: How Fraud, Bias, Negligence, and Hype Undermine the Search for Truth” in 2020. Seems to have weekly column in the i newspaper on same theme. He was at KCL but not sure if he’s still there or a full time writer/journalist now.Is he prominent in some way? He looks pretty young for the image.
Former academic ( resigned from KCL last year). He is probably the only notable UK science commentator currently writing in popular media. Mostly on the ball although he went a bit weird on Geoffrey Hinton's cassandra moment, still he has a flare for connection to common culture not evident in the usual donnish 'speaking from authority' that is UK science commentary:Is he prominent in some way? He looks pretty young for the image.
for those stumped by the idiom >
This sounds bad. Cognitive deficits = anxiety + depression. Of course!
“More than one in three people experiencing long COVID symptoms perceived such cognitive deficits, which have been found to be related to anxiety and depression.
The findings indicate that psychological issues such as anxiety or depressive disorders may play a part in some people who are experiencing long COVID, technically known as post-COVID-19 condition, or PCC.
"This perception of cognitive deficits suggests that affective issues—in this case anxiety and depression—appear to carry over into the long COVID period," said senior author Dr. Neil Wenger, professor of medicine in the division of general internal medicine and health services research at the David Geffen School of Medicine at UCLA. "This is not to say that long COVID is all in one's head, but that it is likely not a single condition and that for some proportion of patients there is likely a component of anxiety or depression that is exacerbated by the disease."
“More than one in three people experiencing long COVID symptoms perceived such cognitive deficits, which have been found to be related to anxiety and depression.
The findings indicate that psychological issues such as anxiety or depressive disorders may play a part in some people who are experiencing long COVID, technically known as post-COVID-19 condition, or PCC.
"This perception of cognitive deficits suggests that affective issues—in this case anxiety and depression—appear to carry over into the long COVID period," said senior author Dr. Neil Wenger, professor of medicine in the division of general internal medicine and health services research at the David Geffen School of Medicine at UCLA. "This is not to say that long COVID is all in one's head, but that it is likely not a single condition and that for some proportion of patients there is likely a component of anxiety or depression that is exacerbated by the disease."
This sounds bad. Cognitive deficits = anxiety + depression. Of course!
“More than one in three people experiencing long COVID symptoms perceived such cognitive deficits, which have been found to be related to anxiety and depression.
The findings indicate that psychological issues such as anxiety or depressive disorders may play a part in some people who are experiencing long COVID, technically known as post-COVID-19 condition, or PCC.
"This perception of cognitive deficits suggests that affective issues—in this case anxiety and depression—appear to carry over into the long COVID period," said senior author Dr. Neil Wenger, professor of medicine in the division of general internal medicine and health services research at the David Geffen School of Medicine at UCLA. "This is not to say that long COVID is all in one's head, but that it is likely not a single condition and that for some proportion of patients there is likely a component of anxiety or depression that is exacerbated by the disease."
Perceived Cognitive Deficits in Patients With Symptomatic SARS-CoV-2 and Their Association With Post–COVID-19 Condition
posted here: https://www.s4me.info/threads/perceived-cognitive-deficits-in-patients-with-symptomatic-sars-cov-2-and-their-association-with-post–covid-19-condition-2023-liu-et-al.33181/
How are they so bad at this? It's the near perfection of this incompetence that is infuriating. Just so completely out of their depth that they can't even see that they are failing miserably.“More than one in three people experiencing long COVID symptoms perceived such cognitive deficits, which have been found to be related to anxiety and depression.
The findings indicate that psychological issues such as anxiety or depressive disorders may play a part in some people who are experiencing long COVID, technically known as post-COVID-19 condition, or PCC.
And just the same way every damn time. They don't know, so they don't want to know. I've never seen professionals so uncurious, so apathetic about knowing things they don't already do. The contrast with the software industry is just staggering.
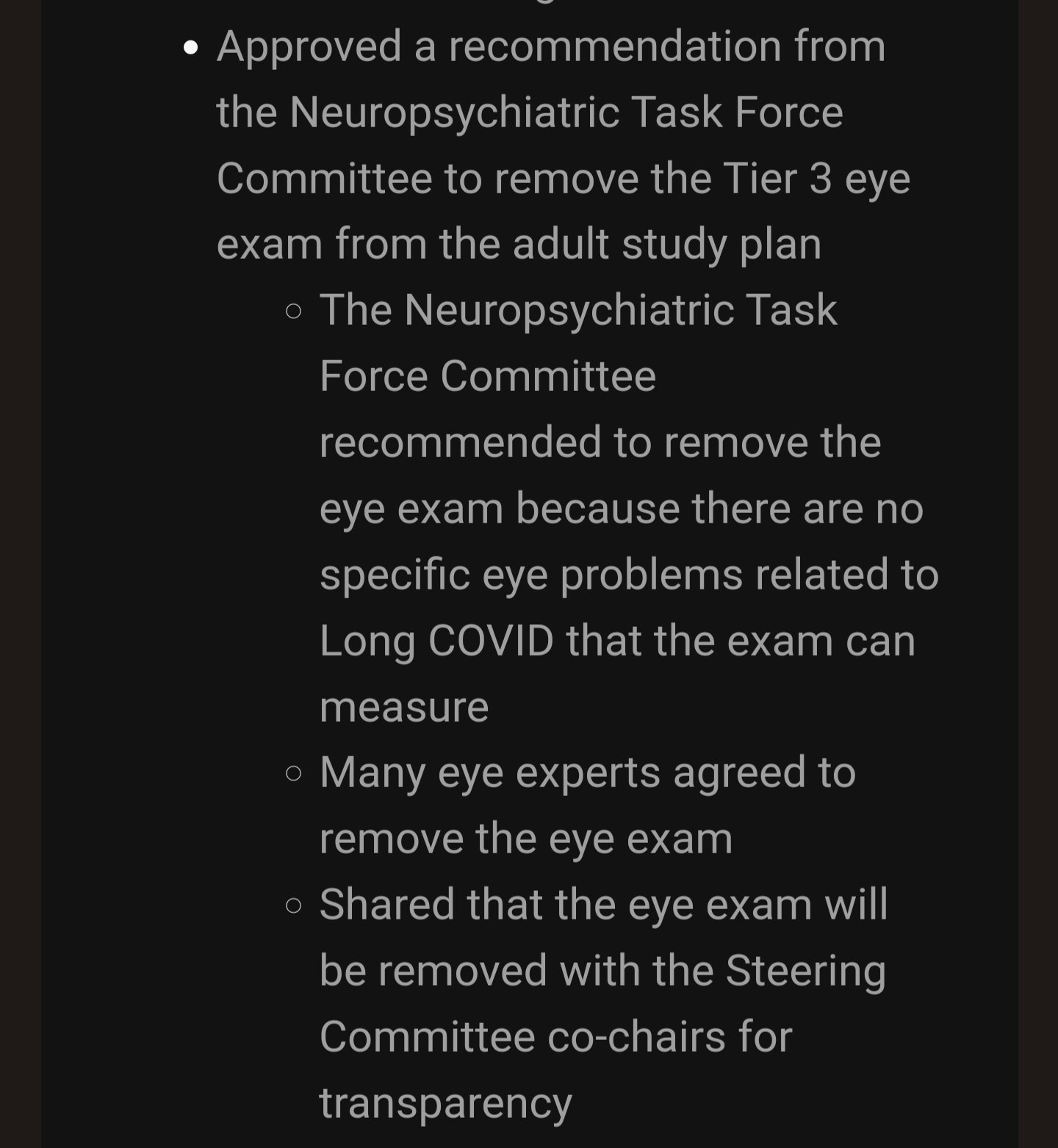
Of course there are many vision issues with LC (and ME). But their standard tests don't show much, so they decided that it doesn't matter. WTF? This isn't ordinary incompetence anymore, this is probably the most extraordinary incompetence. They literally have every chance to succeed, there is not a single obstacle on the way, and they even can't be bothered. It's so bad that the future of health cannot be in the hands of medicine, this entire disaster will have to be bypassed, they just stopped trying entirely.
From:
Last edited by a moderator:
Dakota15
Senior Member (Voting Rights)
Sharing from a local advocacy update in MN, @SunnyK [mods feel free to move, but wanted to share to update]
MN legislation is meeting over the next few days & weeks to determine what is funded & at what level in the omnibus bill. They are meeting to discuss the House version (HF2930) & Senate version (SF2995) of the omnibus bill - and to reconcile differences between the two. Both versions have included proposed language & budget to establish a state-funded Long COVID program in MN.


MN legislation is meeting over the next few days & weeks to determine what is funded & at what level in the omnibus bill. They are meeting to discuss the House version (HF2930) & Senate version (SF2995) of the omnibus bill - and to reconcile differences between the two. Both versions have included proposed language & budget to establish a state-funded Long COVID program in MN.
- The House version only has a one-time appropriation for funding, meaning the Minnesota Department of Health (MDH) would receive state funds for one biennium (fiscal years 2024 and 2025), and $0 thereafter.
- The Senate includes full funding beyond the next biennium. They also added language that would expand the scope of MDH's work to include “related conditions” – post-infection conditions such as ME/CFS and POTS potentially stemming from acute illnesses other than COVID-19 (sharing screenshot on this below).
Last edited:
Some posts have been moved to the News from the World Health Organisation thread.
We have a thread on some of his writing:Is he prominent in some way? He looks pretty young for the image.
Stuart Ritchie, science journalist, articles on science fraud and open science
Ritchie’s inews article can be read without paywall here.
Ritchie’s tentative reference to PACE in a Spectator article is discussed here: https://www.s4me.info/threads/stuar...cles-on-science-fraud-and-open-science.21166/
Hmmm I recently in last six month got into this guys blog so was pleased he’d got a column.
but is this showing a big change of tone to what expected on reading this?
I’m tired so haven’t been able to mentally analyse as I might the points he makes in ridiculousness of listening to patients or re-read Ed Yong or my comments on that one but this really attacks him. Directly. And you don’t do that unless you’ve been given orders/converted or said article really has gone off the rails. And I would have spotted it if that article from Ed was Suddenly off the rails and don’t think it was ?
disheartening if this is a change in mind from this guy so soon after moving if the points he’s picked out and made rather strongly with a lot of incredulity of tone which I don’t like and reminds me of BPS and their belittling tone to suggest another’s half line note was an outrageous suggestion proving their incompetence ha ha . I’d have thought if Ed Yong deserved anywhere near this we’d have picked out some of these ‘howlers’ apparently in there ourselves?
- Status
- Not open for further replies.