Moderator note: This post has been moved from a thread about an article that has been deleted.
____________________
EDITED: I've heavily edited this post for better context now it's been moved from its original location:
This thread is a spin off thread from this thread:
Treating medically unexplained symptoms via improving access to psychological therapy (IAPT): major limitations identified, 2020, Geraghty and Scott
https://www.s4me.info/threads/treat...entified-2020-geraghty-and-scott.13501/page-3
On April 01, 2020, IAPT is scheduled to roll-out its new
IAPT Data Set version 2.0, which will replace
IAPT Data Set v1.5.
This spin off thread contains links for the
IAPT v2.0 Data Set web pages, the October 2019 Stakeholder Consultation pages, documentation, spreadsheets, stakeholder presentation etc.
The stakeholder consultation in October 2019 ran for a month. Following the consultation, some revisions to the draft
Data Set v2.0 and its associated documentation were posted on the Consultation pages.
One of the proposed revisions made after the Consultation was for:
"[An] amendment to the mapping for MUS-Other and replacement of MUS terminology within the document."
This relates to an amendment to the
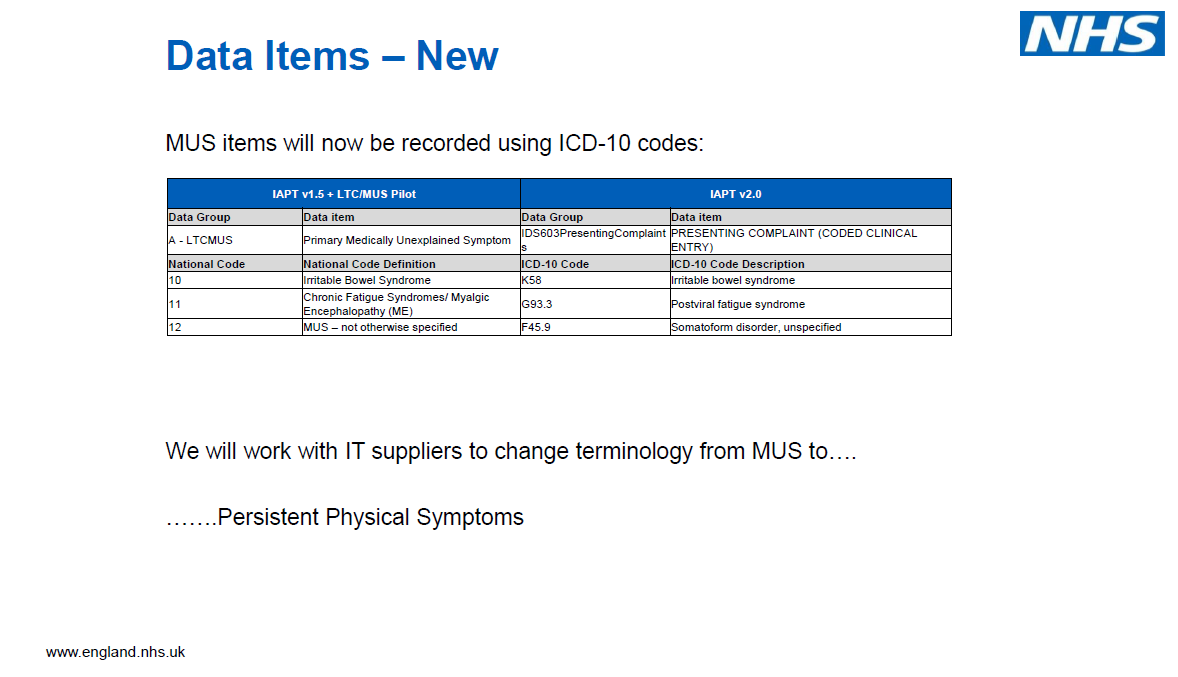
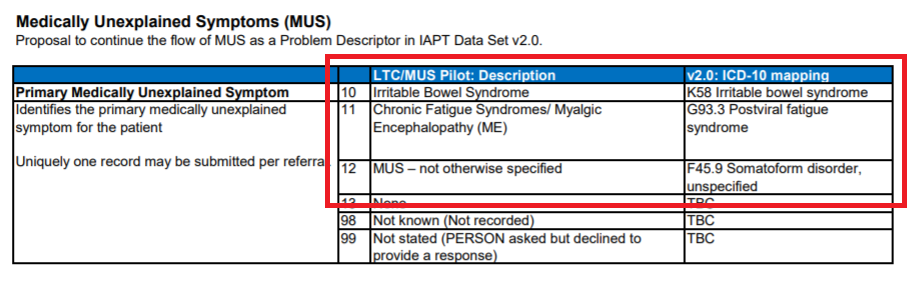
earlier proposed mapping for
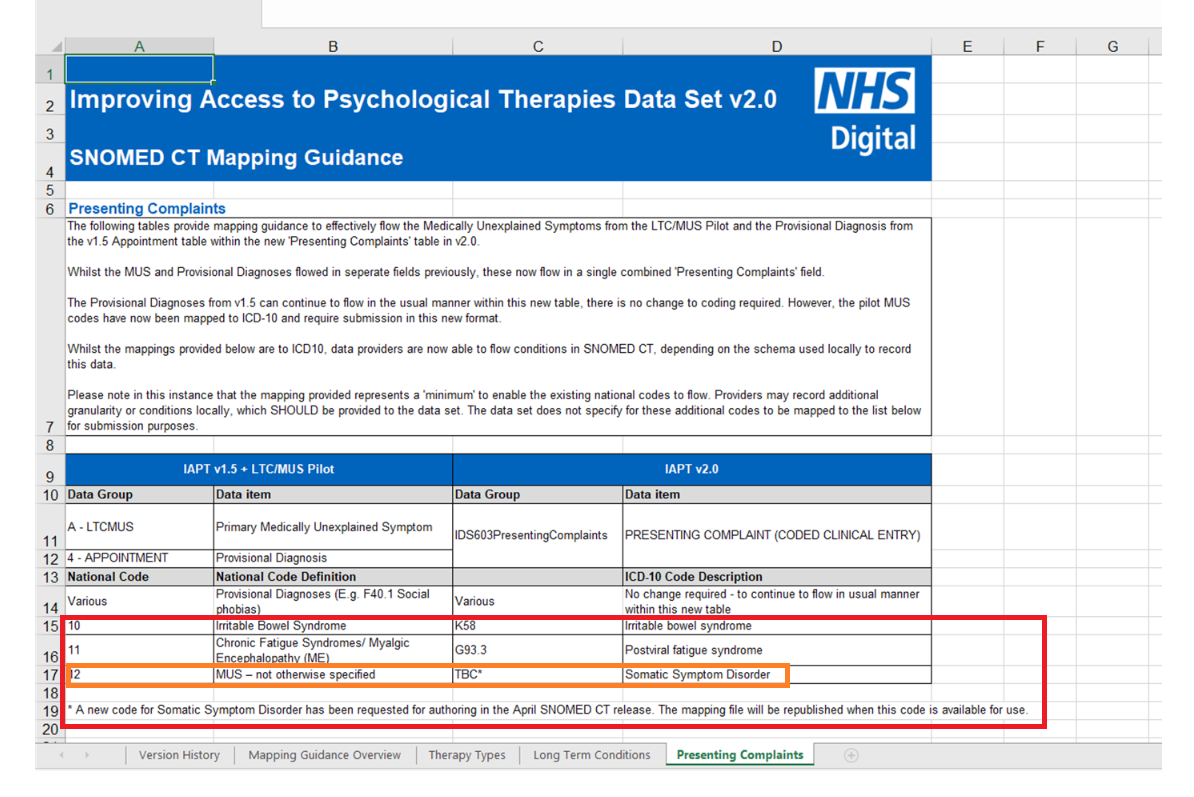
v2.0, as it had appeared in the table immediately, below:
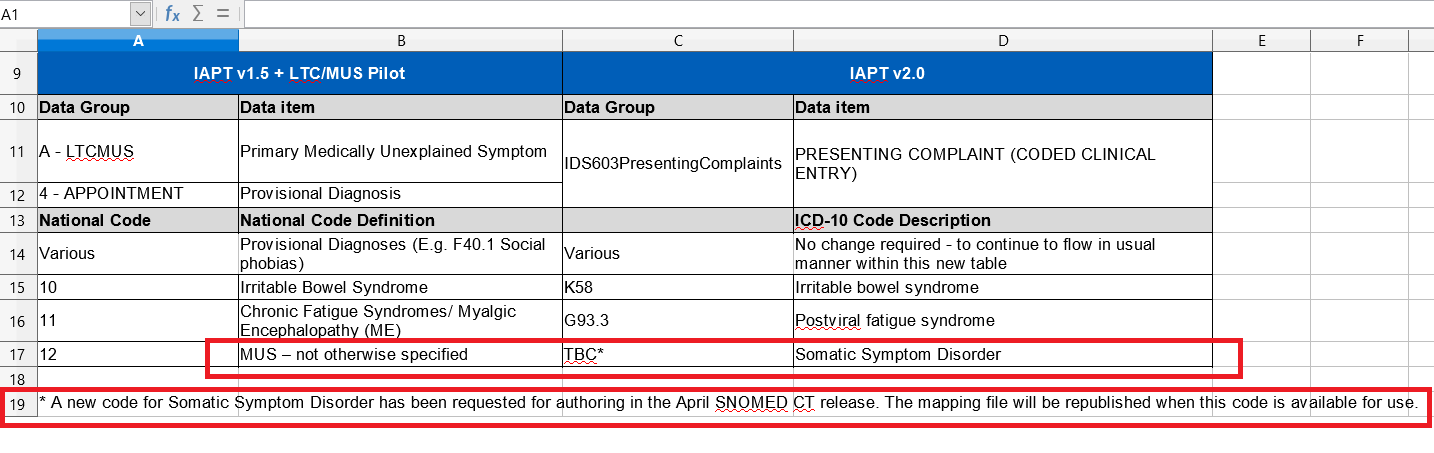
which was revised in November/December to:
Note the new ICD-10 map codes for IBS; and CFS/ME (ie K58 and G93.3 - not F45.x codes).
"MUS - not otherwise specified" is proposed to be mapped to
DSM-5's Somatic symptom disorder, if IAPT's request for a new Concept code for Somatic symptom disorder to be added to the
UK Edition of SNOMED CT is approved.
The request had been discussed in a call between "IAPT senior team" and NHS Digital, on November 11.
Request 29847 was submitted on November 13.
According to the details for
Request 29847, the term "Medically unexplained symptoms" is now considered by IAPT to not be "appropriate" terminology and that DSM-5's Somatic symptom disorder
"is the appropriate definition for this cohort".
The thread contains a
copy of the Request 29847 for addition of Somatic symptom disorder to the SNOMED CT UK Edition, which is marked as "Urgent".
IAPT want to fast track this request for a new Concept code in order to have it implemented in time for inclusion in the forthcoming Data Set v2.0 and to revise the terminology in its associated documentation. The status of the request is designated: "Provisionally approved".
(IAPT is now able to use ICD-10 codes or SNOMED CT UK Edition terminology codes in its data sets and for
Data Set v2.0, will also be making use of many SNOMED CT Concept terms for non medical disorder clinical terminology.)
I don't want to see DSM-5's Somatic symptom disorder being embedded into NHS England via a backdoor marked "IAPT".
The DSM-5 isn't used very much in the UK, and primary care and secondary care specialities will be unfamiliar with the DSM-5 and with the new Somatic symptom disorder diagnostic construct.
The classification and terminology systems that are mandatory for use in NHS England are ICD-10 Version: 2016 and SNOMED CT UK Edition.
Although the WHO has approved the addition of exclusions for PVFS; ME; and CFS under its ICD-11 Bodily distress disorder category, there are no exclusions for these terms for the DSM-5's Somatic symptom disorder.
On February 23, I wrote to NHS Digital terminology leads and Ccd in two SNOMED International's terminology leads, to hopefully throw a spanner in the works by asking,
inter alia:
if the DSM-5's SSD construct is considered by IAPT leads as the
"appropriate definition for this [MUS - not otherwise specified]
cohort", why have they not considered the similarly conceptualised, ICD-11 Bodily distress disorder diagnostic construct - given that DSM-5 is little used in the UK; given that ICD is the mandatory classification system and given that ICD-11 will eventually be adopted by NHS England?
The ICD-11 BDD term already has a Concept code in SNOMED CT that has been mapped to ICD-10
F45.9 Somatoform disorder, unspecified, which is the same code IAPT had planned to use back in November, prior to the amendment to the proposed mapping, for "MUS - not otherwise specified".
I have recommended at the end of my feedback:
"No requests for adding DSM-5 Somatic symptom disorder to SNOMED CT UK Edition should be approved or implemented at this stage. Advice should be sought from the SNOMED CT International Edition terminology team."
Whether the information and points raised within my submission will be enough to stop the request from progressing any further, or delay a decision beyond April in order that the request can be discussed with SNOMED International's terminology leads and with the WHO, I don't know.
There is a very long slide presentation* for professional stakeholders which states in
Slide #71 the intention (prior to the November decision to request a SNOMED CT code for Somatic symptom disorder) to replace "MUS" terminology within documentation with the term,
"Persistent Physical Symptoms".
It is currently unclear whether the intention remains:
a) to revise the
terminology in the documentation to "Persistent Physical Symptoms" and use DSM-5's Somatic symptom disorder as the
Concept code for the map (if the request for addition of SSD to SNOMED CT UK Edition is approved); or
b) to use "Somatic symptom disorder" for
both the revised terminology in the documentation and the
Concept code for the map (if the request for addition of SSD to SNOMED CT UK Edition is approved).
*
IAPT Stakeholder Events, November 2019 - Presentation Slides
https://digital.nhs.uk/binaries/con...eholder_events_november_2019-final-slides.pdf