That is what the BPS crowd will argue, it is just faking or deconditioning.I also have concerns about any possible ability to fake this test, for pwme to be accused of faking or not trying hard enough.
Also as to whether it could be interpreted as deconditioning.
-
Notice: S4ME will have a short interruption of service on May 30. More information here.
You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Hand grip strength as a clinical biomarker for ME/CFS, 2018, Nacul et al
- Thread starter Suffolkres
- Start date
Alvin
Senior Member (Voting Rights)
You would not be able to just use hand grip and say yes patient has ME since many conditions have reduced grip strength. From Parkinsons to Osteoporosis to who knows what reduced grips strength will be a measurable symptom.It's not about lying or not lying. It's about how reliable and accurate this test is, and for places like the NHS, it's also about how cost-effective it is.
If the test isn't very reliable or accurate, then it's easier to just ask the patient if they have PEM and go with that. Why bother with a three-day test when it's no more useful than a questionnaire?
ETA: These are questions and hypotheticals. I'm not necessarily saying the tests are inaccurate.
As i mentioned in another thread Parkinsons has no widely used biomarker, clinicians do tests on patients which i had done on me from from gait, walking, observing and asking about dyskinesias, checking grip strength, cogging, spatial orientation, motor control, muscle strength, questions about sense of smell and even questions about facial expressions if its not observed in the interview. There are other tests that i have forgotten as well. No one suggests patients are faking Parkinsons and why, because its not considered a psychosomatic disease and they have a decent in office testing package. They know its real even if imaging a patient with available technology will not show anything in most cases. The diagnostic test series clinicians are taught are designed to figure out if the patient has Parkinsons and at what stage it is at.
So this is not a matter of a test thats infallible, this is a matter of discrediting the doctors who refuse to do ethical science. By rejecting a test because its not infallible we are only making our paths forward more difficult.
When I was tested for Parkinsons and dementia they found i had many of the symptoms at times from diskinesias to memory issues to reduced grip strength, low muscle strength but i was not mistakenly diagnosed with Parkinsons because the tests were good enough that even though i had many symptoms (especially while PEMed) they could distinguish it based on their training. Also i don't have dementia though they noticed several cognitive issues.
An ME testing package would need testing and verification and its reasonable that grip strength could be part of it though i would only use it on mild patients, at moderate or severe it can cause instant PEM which it would in me today.
Perhaps we could develop one as a forum, from the CCC to some of the physical tests we know about if a team wanted to we could put together a diagnostic series and see if anyone is interested in qualifying it for clinical use. Then again Dr Klimas' clinic may already have something along these lines that they use and could be made clinical practice.
Last edited:
Mithriel
Senior Member (Voting Rights)
The theory goes that when they test muscle strength, people who are faking have a normal grip that suddenly drops because the conscious faking takes longer than if it is real. I often felt that told against someone with ME who could grip normally but not sustain it.
In the 70's or 80's, I read a book I found very interesting. They suggested that handwriting could be used to detect disease early because, among other things, the fine motor control needed showed up muscular deficits much sooner than standard testing. I used to be able to write well for a few sentences until it became illegible further down the page. Nowadays my writing is abysmal and unreadable.
My grip has become very bad as well. My teenage grandson was staying with us and I kept thinking he was putting the lids on things too tightly till I realised I had just stopped being able to open things.
In the 70's or 80's, I read a book I found very interesting. They suggested that handwriting could be used to detect disease early because, among other things, the fine motor control needed showed up muscular deficits much sooner than standard testing. I used to be able to write well for a few sentences until it became illegible further down the page. Nowadays my writing is abysmal and unreadable.
My grip has become very bad as well. My teenage grandson was staying with us and I kept thinking he was putting the lids on things too tightly till I realised I had just stopped being able to open things.
Mithriel
Senior Member (Voting Rights)
Posting this separately.
My husband was at a medical computing conference last week and one of the speakers was very interesting. His company had developed algorithms for the New York stock exchange but now they have turned to medical computing.
They are developing algorithms to detect patterns of disease to give early diagnosis. Their device will pick out patterns of symptoms so it will be most useful for things like migraine and Parkinson's which have no definitive test. They try to make out ME is in a category of it's own because there is no test but it is not unusual that way.
We have a pattern of disease which is unique, that is what things like the ICC try to pick out. If a device that does that becomes commonplace the ordinary doctor may accept ME in the same way as other diseases. As said above, they can't deny a result in our case that is accepted for other diseases.
My husband was at a medical computing conference last week and one of the speakers was very interesting. His company had developed algorithms for the New York stock exchange but now they have turned to medical computing.
They are developing algorithms to detect patterns of disease to give early diagnosis. Their device will pick out patterns of symptoms so it will be most useful for things like migraine and Parkinson's which have no definitive test. They try to make out ME is in a category of it's own because there is no test but it is not unusual that way.
We have a pattern of disease which is unique, that is what things like the ICC try to pick out. If a device that does that becomes commonplace the ordinary doctor may accept ME in the same way as other diseases. As said above, they can't deny a result in our case that is accepted for other diseases.
It's M.E. Linda
Senior Member (Voting Rights)
I read it as three tests on separate days, simply because I was anticipating that it would capture PEM. Three tests on one day would be helpful for cost purposes, but I'm not sure what it's capturing in that case. How quickly does PEM kick in for most of us?
I think it would be useful to know how the study attempts to avoid feigned weakness or lack of volition, because I suspect those will be the first two objections raised to the results. I'm not saying those objections are true, but we should consider them.
My first appointment was last week. The hand grip test was using the hand machine three times with a pause in between each go. I felt as if my number 2 and 3 grips were tighter, because I had got used to the machine.
My highest result was about 5kg lower than the “weak” average of a woman my age (according to a random scale I found online)
Each occasion my grip recorded 2kg lower than the previous.
adambeyoncelowe
Senior Member (Voting Rights)
That's very interesting! Thanks for sharing.My first appointment was last week. The hand grip test was using the hand machine three times with a pause in between each go. I felt as if my number 2 and 3 grips were tighter, because I had got used to the machine.
My highest result was about 5kg lower than the “weak” average of a woman my age (according to a random scale I found online)
Each occasion my grip recorded 2kg lower than the previous.
Suffolkres
Senior Member (Voting Rights)
Don't forget that this team also have been involved in evaluation of MS against ME ( Norfolk/Suffolk/London) - published this recently.
https://link.springer.com/article/10.1007/s41669-018-0071-6
Functional Status and Well-Being in People with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Compared with People with Multiple Sclerosis and Healthy Controls
https://link.springer.com/article/10.1007/s41669-018-0071-6
Functional Status and Well-Being in People with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Compared with People with Multiple Sclerosis and Healthy Controls
- Caroline C. Kingdon

- Erinna W. Bowman
- Hayley Curran
- Luis Nacul
- Eliana M. Lacerda
dangermouse
Senior Member (Voting Rights)
In the 70's or 80's, I read a book I found very interesting. They suggested that handwriting could be used to detect disease early because, among other things, the fine motor control needed showed up muscular deficits much sooner than standard testing. I used to be able to write well for a few sentences until it became illegible further down the page. Nowadays my writing is abysmal and unreadable.
My writing was/is affected, also my ability to do artwork as I can’t hold pens/pencils etc comfortably and dexterity is shocking.
My writing is very hit and miss now, mostly miss. I can sometimes write half a sentence in half decent style, any attempt after that isn’t at all legible.
Inara
Senior Member (Voting Rights)
I made that test for a treatment study, once at the start and once at the end.
At the start, my handgrip strength was lower than normal (I was told at the end of the study), at the end it was much much better than normal.
At the start, the handgrip strength got slightly worse with repetition (here also: 3 repetitions), at the end, with every repetition I got better. (Like with resistance training, I had the feeling with knowing how it works I got better - although I don't think that explains the improvement alone.)
I am very curious to see those results, now with that Nacul-paper out. Will there be a replication, I wonder?
At the start, my handgrip strength was lower than normal (I was told at the end of the study), at the end it was much much better than normal.
At the start, the handgrip strength got slightly worse with repetition (here also: 3 repetitions), at the end, with every repetition I got better. (Like with resistance training, I had the feeling with knowing how it works I got better - although I don't think that explains the improvement alone.)
I am very curious to see those results, now with that Nacul-paper out. Will there be a replication, I wonder?
Last edited:
adambeyoncelowe
Senior Member (Voting Rights)
Yes, that's a good point. If I prepare myself, I can blow significantly better than normal. And as I went to drama school (I missed Mel B by a few years, but Jack P Shepherd was in my sister's class) I can put a lot of power into my lungs via my diaphragm. That can throw off the readings. But it's probably still a useful tool, if used with other things.They use peak flow meters to measure for asthma and this seems similar to me. Useful, potentially, but also not a perfect measure.
I have unusually large lungs. Have not done a spirometry test for decades, but when young and healthy I scored well above age predicted results. Even now, after 35 years of ME, I would do at least okay for my age on spirometry, and maybe better than that. So that measure could be misleading in my case.Yes, that's a good point. If I prepare myself, I can blow significantly better than normal. And as I went to drama school (I missed Mel B by a few years, but Jack P Shepherd was in my sister's class) I can put a lot of power into my lungs via my diaphragm. That can throw off the readings. But it's probably still a useful tool, if used with other things.
My handwriting, however, has gone to shit. Though how much of that is due to simple lack of practice from living in the computer and keyboard age is unclear.
I did a grip strength test early into my disease, when i had a functional assessement done. While i do not remember the numbers associated with my grip strength, i still remember the deep brain pain it gave me after every attempts to grip as hard as i could.
This test may not be very specific to our condition, and it would still have the potential to cause PEM just like an exercise test.
I am hoping for a blood test.
This test may not be very specific to our condition, and it would still have the potential to cause PEM just like an exercise test.
I am hoping for a blood test.
NelliePledge
Senior Member (Voting Rights)
This isn’t specific to ME but if it is a reasonably widely used measure of muscle weakness/indicator of frailty and we want ME to be seen in context with other comparable chronic illnesses why would we not use this. I’m not saying including this in list of tests in NICE guidelines would be revolutionary but wouldnt it help a little to making ME be seen as more like say MS than like say anxiety.
weirdly when I had my "medical examination" for my critical illness insurance claim the "Doctor" had me do a grip strength test. This was the only actual physical test that I did and the rest of the time was just spent asking me questions. He didn't say why he was carrying out this test. Then in his report to the insurance company he lists the results and puts a nice graph in but nowhere does he say what this means or why he did it. So to me it seemed completely irrelevant but maybe he was doing it just to collect data for himself or something weird like that.
Andy
Senior Member (Voting rights)
As well as;Don't forget that this team also have been involved in evaluation of MS against ME ( Norfolk/Suffolk/London) - published this recently.
https://link.springer.com/article/10.1007/s41669-018-0071-6
Functional Status and Well-Being in People with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Compared with People with Multiple Sclerosis and Healthy Controls
That research continues, is ongoing up till 2020 or so.
- Caroline C. Kingdon
- Erinna W. Bowman
- Hayley Curran
- Luis Nacul
- Eliana M. Lacerda
Prevalence of and risk factors for severe cognitive and sleep symptoms in ME/CFS and MS. http://researchonline.lshtm.ac.uk/3983828/
Differing case definitions point to the need for an accurate diagnosis of myalgic encephalomyelitis/chronic fatigue syndrome. http://researchonline.lshtm.ac.uk/4646053/
How have selection bias and disease misclassification undermined the validity of myalgic encephalomyelitis/chronic fatigue syndrome studies? http://researchonline.lshtm.ac.uk/3615850/
I also understand that they have another three papers due out in the new year.
DigitalDrifter
Senior Member (Voting Rights)
When I was in a general hospital in 2013, the physiotherapist tested my hand grip strength. When I asked why won't he test me again in a few days or a week to prove deterioration and that I objectively have something wrong with me, he said I would be accused of not trying hard enough.I'm just imagining them accusing us of not trying hard enough to grip because of some sort of fear avoidance.
MSEsperanza
Senior Member (Voting Rights)
Full text now available:
https://www.frontiersin.org/articles/10.3389/fneur.2018.00992/full
https://www.frontiersin.org/articles/10.3389/fneur.2018.00992/full
adambeyoncelowe
Senior Member (Voting Rights)
So I've read the study and so it seems like the protocol is to conduct three tests, 30 seconds apart.
ME mild/moderate (MEmm) patients show a significant decline between first and second test (sharper than MS) but a slight increase again by the third test.
Severely affected (MEsa) patients continue to decline even by the third test, and their results are significantly lower than MS and MEmm.
Patients with chronic fatigue that doesn't meet ME criteria (CF/non-ME) score almost as well as healthy controls.
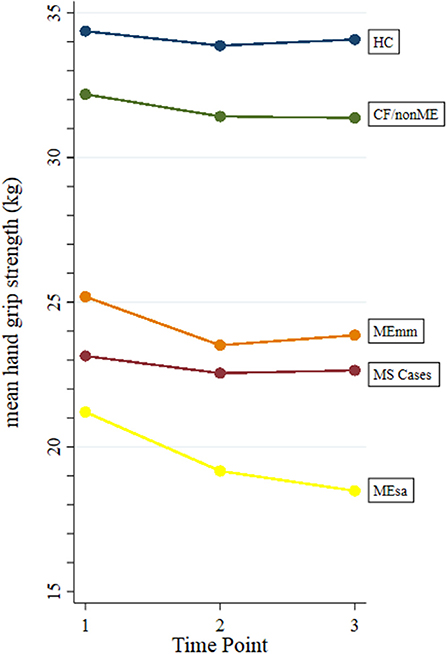
The HGS is used with the SF-36V2 to confirm fatigue and muscle weakness. So it's combining a subjective measure (questionnaire) with a more objective one (HGS test).
ME mild/moderate (MEmm) patients show a significant decline between first and second test (sharper than MS) but a slight increase again by the third test.
Severely affected (MEsa) patients continue to decline even by the third test, and their results are significantly lower than MS and MEmm.
Patients with chronic fatigue that doesn't meet ME criteria (CF/non-ME) score almost as well as healthy controls.
The HGS is used with the SF-36V2 to confirm fatigue and muscle weakness. So it's combining a subjective measure (questionnaire) with a more objective one (HGS test).