@rvallee I needed to go out first thing this morning and didn't have time to give you a fuller response. But here it is:
Isn't the UK adopting the SNOMED changes classifying it within neurology?
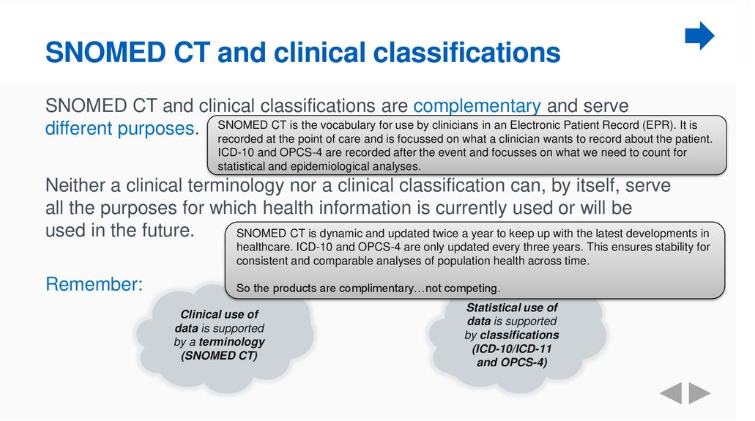
SNOMED CT terminology system isn't structured into a series of chapters like ICD-10 or ICD-11.
SNOMED CT Concepts (unique, coded, machine readable terms) are defined by their relationship with other SNOMED CT Concepts.
Any given Concept (SCTID) term may be assigned a number of parents (known as "supertypes") which might span more than one chapter or more than one category block in ICD.
As an example,
SCTID 127346000 | Neurologic disorder of eye movements (disorder) is assigned the
Disorder or nervous system parent but is also defined by its relationship with all of the following parent Concepts:
Disorder of body system (disorder)
Finding by site (finding)
Eye / vision finding (finding)
Visual system disorder (disorder)
Disorder of eye movements (disorder)
Disease (disorder)
Clinical finding (finding)
Finding by site (finding)
Disorder by body site (disorder)
Disorder of body system (disorder)
Disorder of nervous system (disorder)
ICD-11 has moved in the direction of also defining ICD category terms by more than one parent, by introducing secondary and tertiary parenting.
For ICD-11, all categories are assigned to a "primary parent" chapter, but in some cases, a category may be secondary parented under a second chapter, or be assigned under an additional parent class within the "primary parent" chapter (aka the Linearization parent).
This means that for ICD-11, for example, skin neoplasms can be listed under both
Chapter 14 Diseases of the skin and
Chapter 04 Neoplasms.
So for SNOMED CT, CFS isn't classified "within neurology", as such, but is assigned these parent Concepts:
Disease (disorder)
Finding by site (finding)
Disorder by body site (disorder)
Disorder of body system (disorder)
Disorder of nervous system (disorder)
whereas before the change was approved, it was assigned only these two parents (because the
Multisystem disorder Concept term had been retired across the entire terminology system for the January 2018 release of the International Edition):
Disease (disorder)
Finding by site (finding)
Continued in next post.