Hello, welcome.
This idea of anxious / depressive / perfectionist types is based on outdated psychological research ideas. But common misconception among neurologists who mostly don’t know much about ME/CFS and like to throw out these ideas as facts!
Thanks!
So what to make of this study then?
https://pubmed.ncbi.nlm.nih.gov/36069885/ - quite a strong association of pre-COVID distress and long COVID. I am aware that long COVID is not necessarily identical to ME/CFS but I think that a subset of long COVID patients could be classified as having ME/CFS.
Hi
@desmolysium, thanks for your interest in ME/CFS.
A couple of us have been discussing epigenetic changes in the brain in relation to a recent autopsy study presentation (data not published yet). The thread may be of interest to you:
- All in all, the HPA axis with the dramatic reduction of CRH-producing neurons in the hypothalamus, a shutdown of the pituitary, and lower cortisol levels found appeared to be pretty much of a wreck in these autopsied patients.
It's a narrative that has been around in ME/CFS for a long time. There's plenty of evidence to the contrary, most recently Leonard Jason's prospective post-EBV study that found no predictive association with baseline anxiety, depression or coping.
Once we know the disease mechanism it may be possible to understand how it contributes to disease in some cases. At our current level of understanding, though, I tend to find that speculating on the role of depression/anxiety/pre-existing mental illness does more harm than good.
I was part of the IMPACC consortium that did longitudinal tracking of people hospitalized with SARS-CoV-2. One of the papers from the group (which I wasn't an author on) looked at acute-phase viral load and long term outcome:
Post-acute sequelae of SARS-CoV-2 (PASC) is still not well understood. Here the authors provide patient reported outcomes from 590 hospitalized COVID-19 patients and show association of PASC with higher respiratory SARS-CoV-2 load and circulating antibody titers, and in some an elevation in...

www.nature.com
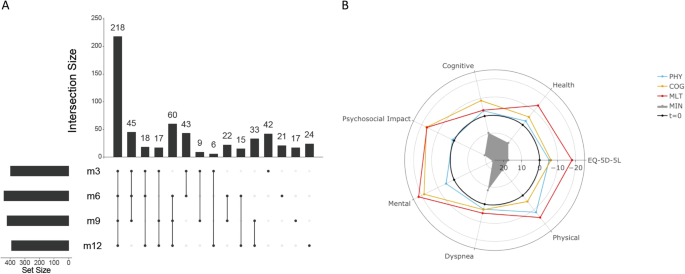
From Fig S4:
View attachment 30943
These plots show qPCR measurements for viral load. The groups there are recovered/minimally affected (MIN), primarily physical deficit (PHYS), primarily cognitive deficit (COG), and physical + cognitive deficit (MLT). The MLT group is the one with functional assessment scores closest to typical ME/CFS cases (with the caveat that a couple people in that group had pre-existing cardiac conditions). From what I remember, this serological data was pretty consistent with nasal swab and antibody titer trends.
Viral load was significantly higher at hospital admission for ppts who went on to have a post-COVID functional deficit, but you can see it's a small difference with a lot of overlap. There's a slight difference at ~day 14, mostly driven by a few outliers. In general, it seems like the people who went on to get LC did not have higher viral titers for much longer than people who recovered--though it may have been an additional risk factor for a handful of cases. Some caveats, obviously, with this being on all hospitalized patients
Very interesting thanks. The "loss of a specific subset of key neurons" is what I mentioned in my article. This is an uncomfortable possibility. There is also preliminary evidence in rodent studies that in diet-induced obesity POMC neurons die (the key subset of neurons that controls energy homeostasis) because of an influx of excessive levels of satiety signals and/or inflammation, which could at least contribute to the permanent setpoint shift in obesity. Is it possible that some neurons in the hypothalamus and/or brain stem are driven into excitotoxicity (or other forms of toxicity) from the infection itself and/or cellular or humoral immune response? But great article, thanks for sharing.
Also, thanks for the info regarding viral load and/or clearance duration. It is surely an additional risk factor but perhaps much weaker than I had suggested.
Interesting though are the trials on metformin on COVID infection. There are 2 trials (if I remember correctly) that show that if metformin is given at the onset of infection, long COVID rates are reduced by almost half - at least in insulin resistant individuals. Metformin presumably does reduce cytokine levels and may also affect mTOR and/or autophagy.
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaf700/8444410
https://pubmed.ncbi.nlm.nih.gov/37302406/
So, what does metformin do to reduce the incidence of LC/ME/CFS?
There is also unpublished data from online surveys by Matt Kaeberlein that people who took rapamycin for longevity purposes have lower rates of LC development than people on the same forums who do not take it. However, many confounders, I am sure. Mechanistically rapamycin and metformin share common intracellular end pathways.
Welcome desmolysium, it's great to be able to chat with you directly.
The comparison with an obesity set-point has occurred to me too and I do find it compelling. The way my system seems to claw back any temporary improvement I have does make it feel like that's my body's new idea of normal.
I had not heard of epigenetic editing before so that was very interesting. Appreciate you taking an interest and sharing your thoughts!
I definitely think the setpoint theory is worth exploring. Also, worth distinguishing whether the new setpoint is changable in theory (as is the case with epigenetic modification) or whether the new "setpoint" is due to neuronal death.
Also I can kind of see why doctors might think they're seeing 'anxiety' when a patient is breathing erratically or seems to be distracted or finding it hard to organise their words, when actually it's physical distress and/or cognitive impairment. Or they think they're seeing 'depression' when it's actually exhaustion.
Totally agree. The neurologist I talked to said that 90% of his colleagues do not even believe that ME/CFS exists, mostly because thus far no real biomarkers had been found other than the reduced VO2 max at the time of PEM. However, I do not know too much about it.
I think that a proper biomarker for the disease would 1) help more doctors believe in the disease (as they have something tangible) and 2) would also potentially help prognostically as to telling us whether a treatment does help. However, easier said than done and I am sure many researchers had been looking for one already. So, are there any proper biomarkers I am not aware of?
Great to have you here
@desmolysium and thanks for joining! I hope you’re able to stick around and get involved.
There’s some really interesting ideas coming out of some of the genetics studies as well as research by a few other groups and I’m sure people be happy to point you in the right direction if you’re interested. Some of the researchers responsible also take part in discussions here and it would be great to have your input too.
The one friend of mine that got ME/CFS has both allergies and also constantly got herpes sores all his life. So there may be something with his immune system that may have potentially increased his risk for developing ME/CFS.
Is there an association between herpes virus reactivation before ME/CFS and the development of ME/CFS? Is there an association with atopy?
In the setpoint hypothesis (as I imagine it), interferons definitely have a central role in how the setpoint is entrained (presumably through epigenetic modifications). But again, just a hypothesis.
Thanks all for the comments.

 desmolysium.com
desmolysium.com
")