John Mac
Senior Member (Voting Rights)
Now published - post with link here
Preprint
Abstract
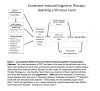
Purpose: Long COVID brain fog is often disabling. Yet, no empirically-supported treatments exist. This study′s objectives were to evaluate feasibility and efficacy, provisionally, of a new rehabilitation approach, Constraint-Induced Cognitive Therapy (CICT), for post-COVID-19 cognitive sequelae.
Design: Sixteen community-residents ≥ 3-months post-COVID-19 infection with mild cognitive impairment and dysfunction in instrumental activities of daily living (IADL) were enrolled. Participants were randomized to Immediate-CICT or treatment-as-usual (TAU) with crossover to CICT. CICT combined behavior change techniques modified from Constraint-Induced Movement Therapy with Speed of Processing Training, a computerized cognitive-training program. CICT was deemed feasible if (a)≥80% of participants completed treatment, (b) the same found treatment highly satisfying and at most moderately difficult, and (c) <2 study-related, serious adverse-events occurred. The primary outcome was IADL performance in daily life (Canadian Occupational Performance Measure). Employment status and brain fog (Mental Clutter Scale) were also assessed.
Results: Fourteen completed Immediate-CICT (n=7) or TAU (n=7); two withdrew from TAU before their second testing session. Completers were [M (SD)]: 10 (7) months post-COVID; 51 (13) years old; 10 females, 4 males; 1 African American, 13 European American. All the feasibility benchmarks were met. Immediate-CICT, relative to TAU, produced very large improvements in IADL performance (M=3.7 points, p<.001, d=2.6) and brain fog (M=-4 points, p <.001, d=-2.9). Four of five non-retired Immediate-CICT participants returned-to-work post-treatment; no TAU participants did, p=.048.
Conclusions: CICT has promise for reducing brain fog, improving IADL, and promoting returning-to-work in adults with Long COVID. Findings warrant a large-scale RCT with an active-comparison group.
https://www.medrxiv.org/content/10.1101/2024.07.04.24309908v1
Preprint
Abstract
Purpose: Long COVID brain fog is often disabling. Yet, no empirically-supported treatments exist. This study′s objectives were to evaluate feasibility and efficacy, provisionally, of a new rehabilitation approach, Constraint-Induced Cognitive Therapy (CICT), for post-COVID-19 cognitive sequelae.
Design: Sixteen community-residents ≥ 3-months post-COVID-19 infection with mild cognitive impairment and dysfunction in instrumental activities of daily living (IADL) were enrolled. Participants were randomized to Immediate-CICT or treatment-as-usual (TAU) with crossover to CICT. CICT combined behavior change techniques modified from Constraint-Induced Movement Therapy with Speed of Processing Training, a computerized cognitive-training program. CICT was deemed feasible if (a)≥80% of participants completed treatment, (b) the same found treatment highly satisfying and at most moderately difficult, and (c) <2 study-related, serious adverse-events occurred. The primary outcome was IADL performance in daily life (Canadian Occupational Performance Measure). Employment status and brain fog (Mental Clutter Scale) were also assessed.
Results: Fourteen completed Immediate-CICT (n=7) or TAU (n=7); two withdrew from TAU before their second testing session. Completers were [M (SD)]: 10 (7) months post-COVID; 51 (13) years old; 10 females, 4 males; 1 African American, 13 European American. All the feasibility benchmarks were met. Immediate-CICT, relative to TAU, produced very large improvements in IADL performance (M=3.7 points, p<.001, d=2.6) and brain fog (M=-4 points, p <.001, d=-2.9). Four of five non-retired Immediate-CICT participants returned-to-work post-treatment; no TAU participants did, p=.048.
Conclusions: CICT has promise for reducing brain fog, improving IADL, and promoting returning-to-work in adults with Long COVID. Findings warrant a large-scale RCT with an active-comparison group.
https://www.medrxiv.org/content/10.1101/2024.07.04.24309908v1
Last edited by a moderator: