Sid
Senior Member (Voting Rights)
Who does the 'deeming' on these assessments of harm and 'whether it was related'?
Trial investigators themselves.
Who does the 'deeming' on these assessments of harm and 'whether it was related'?
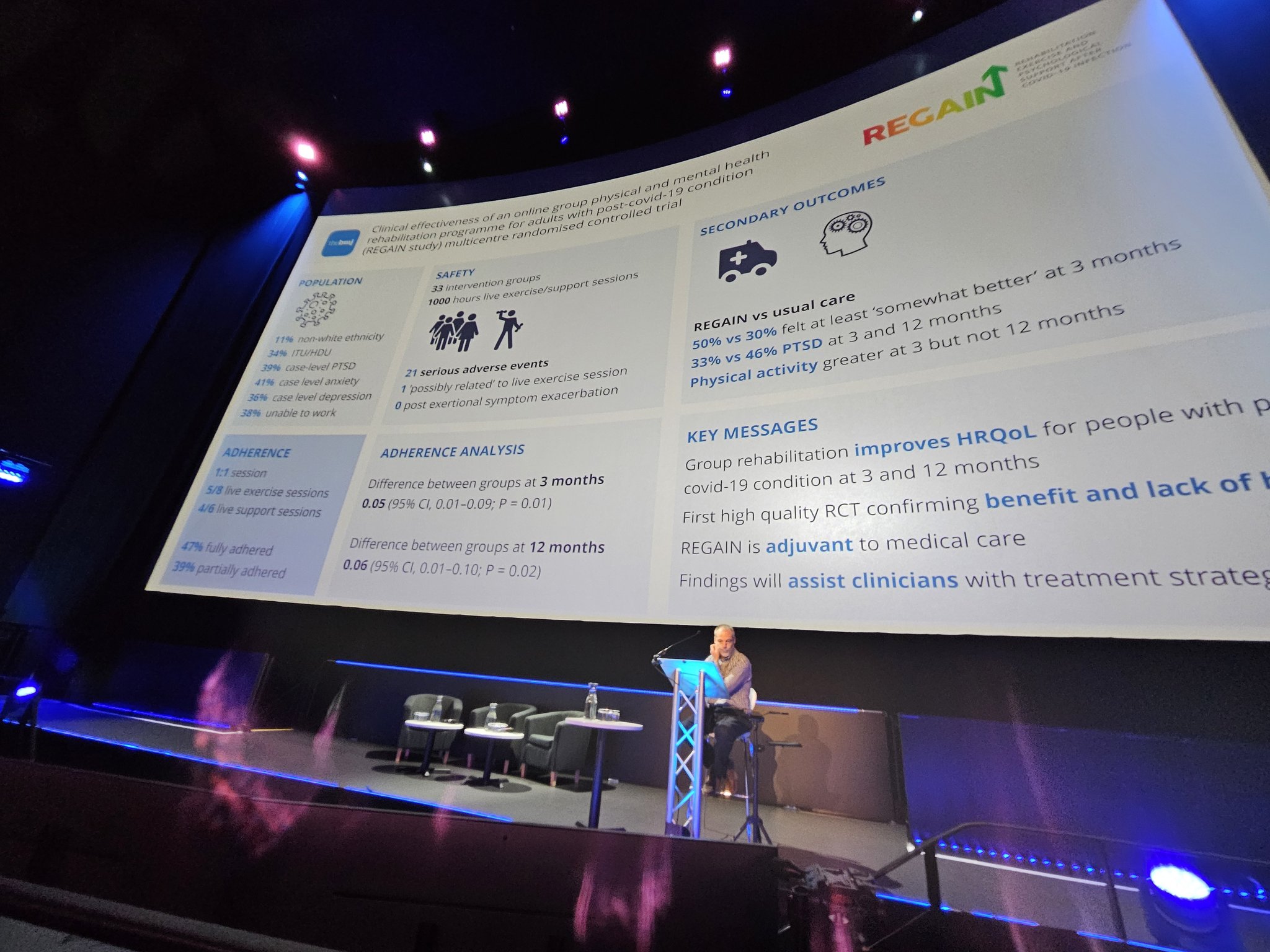
The first funny thing about bringing #PEM into this argument is that THE AUTHORS OF THE STUDY DID NOT. Yep, that's right. One of the cardinal symptoms of #LongCOVID, that is known to be behaviorally and physiologically DISTINCT from fatigue. A symptom that every patient population and serious LC researcher has been publishing as THE symptom to ask about before any exercise or rehab interventions are attempted and these authors didn't ask about it. Didn't. Ask.
the full adherence rate of this clinical trial was less than 50%. Yet they refer to the adherence of their study as "good". Wow. Side note: my whole job for the last decade has been to run clinical trials, including being a PI on some of the largest multi-site rehab trials in stroke out there right now. If FULL adherence to a protocol (in this case defined as showing up to at least 2/3 of the sessions) dips below 80% in our trials we start to wonder what is going on and whether or not the intervention has any mainstream feasibility in the population we have selected because if you can't get more than 80% of people in a clinical trial to stick to a protocol that they're likely receiving money to follow and you have a clinical team being paid to keep them on target, then it is kind of futile to think that in a real-life clinical setting your intervention will be tolerated. So, at 80% we're concerned, at 70% we're downright worried. This team hit 47% and called it "good". I mean...editors @bmj_latest - you all on sabbatical? You ok with calling 47% adherence "good" and publishing it?
Didn't screen for a cardinal symptom of the disease state they're supposedly studying, couldn't get a majority of study participants to follow the interventional protocol (), anything else? Oh yeah: only recruited people who were hospitalized with acute #COVID into their #LongCOVID cohort.
if you were hospitalized with acute COVID and diagnosed with #LongCovid, you should be studied distinctly from #pwLC who were not hospitalized with acute infection because there are likely elements of your pathology that differ from those who were not hospitalized. #pwLC who were hospitalized with their acute illness make up less than 10% of all folks in the world with #LongCOVID.
As such, good authors studying this cohort would make a point to limit the findings of their study, right? Seems like the ethical thing to do, right? Their conclusion:
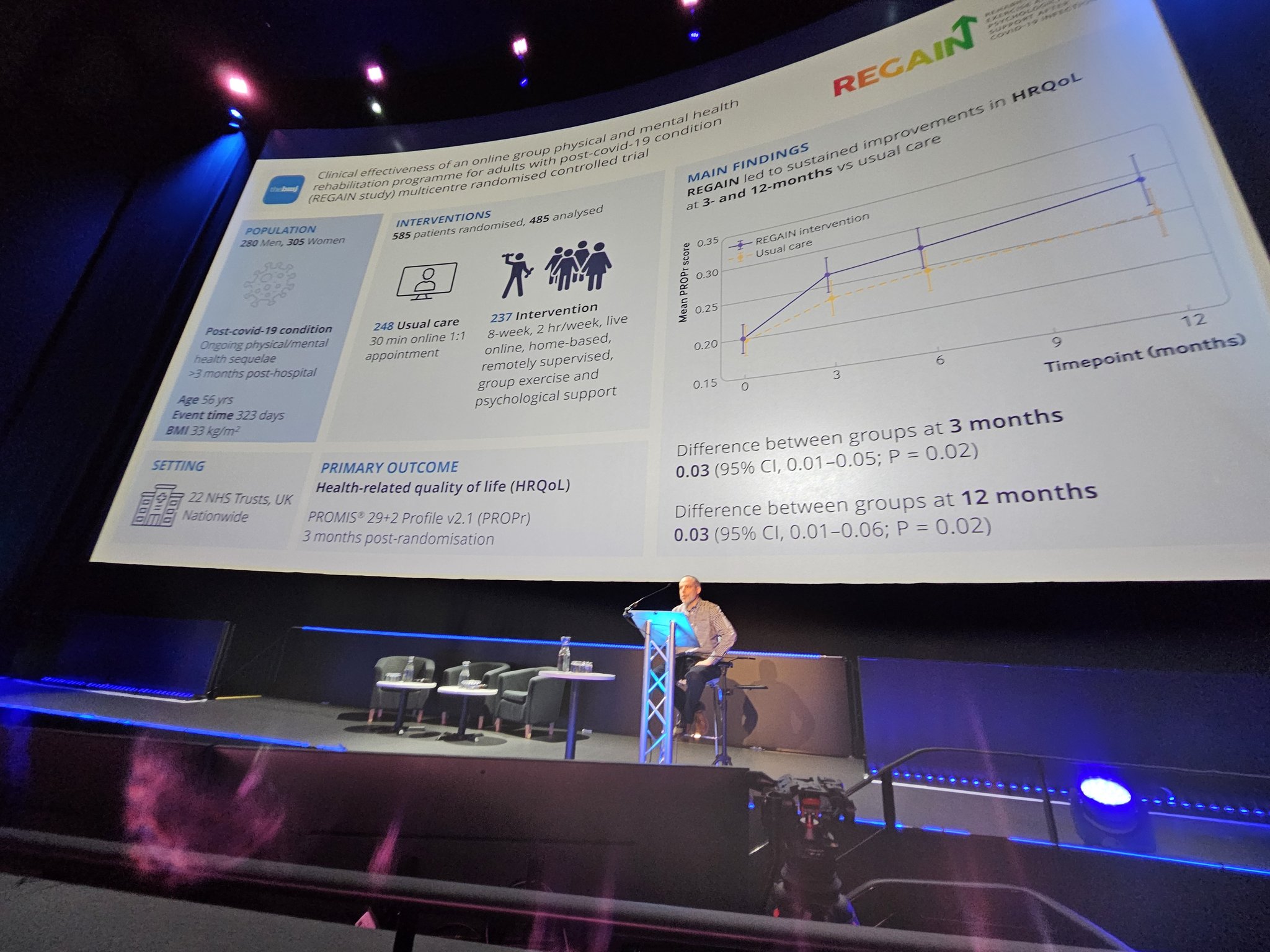
"In adults with post-covid-19 condition, an online, home based, supervised, group physical and mental health rehabilitation programme was clinically effective...."
Once again, I ask: @bmj_latest editors - you asleep at the wheel letting a conclusion like this through? What exactly is going on that you allow a research finding in such a narrow subset of a disease population to be generalized to the entire #LongCOVID population in the conclusions with no pushback? Bad science, worse editorial management.
#pwLC deserve research into interventions that are going to seriously move the needle on what is possible for them. They do not need another tired paper that, if it were honest, would say: "in a cohort of pwLC that represents less than 10% of the total #LongCOVID community, our intervention featuring nothing new that was tolerated by less than 50% of patients seemed to maybe reduce fatigue by 20% or less".
Full letter can be seen here, https://meassociation.org.uk/2024/02/new-scientist-on-the-use-of-exercise-therapy-for-long-covid/Dr Nicola Clague-Baker on Twitter
"A heavily edited letter that we produced in response to the New Scientist article - https://newscientist.com/letter/mg26134790-900-on-the-use-of-exercise-therapy-for-long-covid/"
On the use of exercise therapy for long covid
Published 21 February 2024
From Charles Shepherd, honorary medical adviser, ME Association; Sonya Chowdhury, CEO of Action for ME; and Nicola Baker at the University of Liverpool, UK
You report on the use of exercise for long covid. This condition and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) have some important clinical and pathological overlaps and a significant proportion of people with long covid also meet diagnostic criteria for ME/CFS (17 February, p 14).
In new guidelines on ME/CFS in 2021, England’s National Institute for Health and Care Excellence decided to no longer recommend graded exercise therapy – fixed, incremental hikes in activity – but to recommend activity and energy management based on pacing, staying at levels that feel right for the individual. This followed a thorough review of all the clinical trials that had involved exercise therapy. People with ME/CFS have been harmed by exercise programmes. We hope those with long covid won’t experience the same fate.
https://www.newscientist.com/letter/mg26134790-900-on-the-use-of-exercise-therapy-for-long-covid/
I don't know much about minimally clinically important differences but the idea looks confused to me.
Anyone who tries to define "minimally clinically important differences" based on some statistical definition, related to the standard deviation or other measure affected by signal-to-noise ratio of the scale is a charlatan.
he even included the truncated axis that is a thing only done shadily