Dx Revision Watch
Senior Member (Voting Rights)
NHS Clinical Networks
Non-Dementia Pathways Guidance from the London Dementia Clinical Networks
January 2020 (Version 2)
PDF: https://www.england.nhs.uk/london/w.../8/2019/07/Final-non-dementia-pathways-V2.pdf
Selected extracts:
The aim of this document is to provide commissioners and clinicians in memory services and primary care with guidance on the appropriate pathways for patients who present with memory complains [sic] due to a range of non-dementia causes
Introduction
The 2019 London memory service audit looked at 988 case notes across 20 services. In addition to finding considerable variation between services; the audit found that overall 40% of patients were not given a diagnosis of dementia and 85% of patients under the age of 65 were not given a diagnosis of dementia
Slide #3:
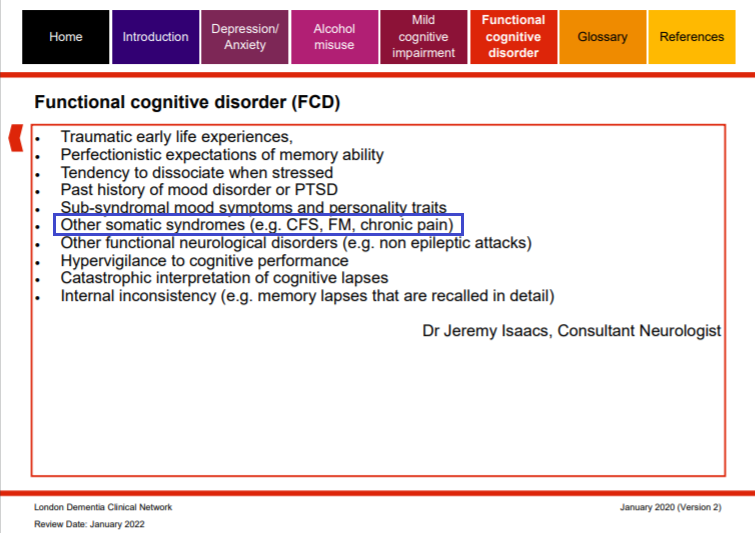
Slide #7
Functional cognitive disorder (FCD)
[Ed: For ICD-11, Dissociative neurological symptom disorder, with cognitive symptoms is coded at 6B60.9 as a child category under parent class: 6B60 Dissociative neurological symptom disorder.]
Slide #25 (My blue highlighting)
Primary care
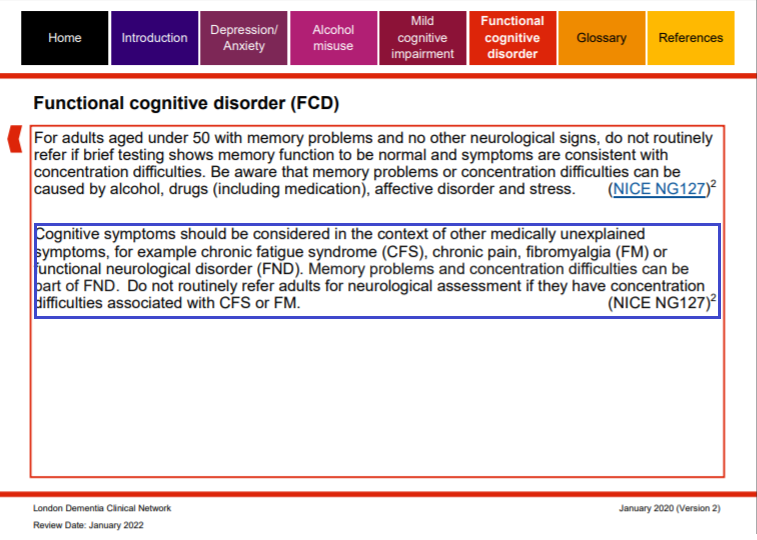
[Ed: NICE NG127 = Suspected neurological conditions: recognition and referral NICE guideline [NG127] Published date: May 2019 Last updated: July 2019 https://www.nice.org.uk/guidance/ng127]
Slide #26 (My blue highlighting)
MAS triage
Slide #28
Diagnostic and post diagnostic pathway

Slide #29 (My blue highlighting)
FCD Flags
Slide #30
Case study

PDF URL (and attached below): https://www.england.nhs.uk/london/w.../8/2019/07/Final-non-dementia-pathways-V2.pdf
Non-Dementia Pathways Guidance from the London Dementia Clinical Networks
January 2020 (Version 2)
PDF: https://www.england.nhs.uk/london/w.../8/2019/07/Final-non-dementia-pathways-V2.pdf
Selected extracts:
The aim of this document is to provide commissioners and clinicians in memory services and primary care with guidance on the appropriate pathways for patients who present with memory complains [sic] due to a range of non-dementia causes
Introduction
The 2019 London memory service audit looked at 988 case notes across 20 services. In addition to finding considerable variation between services; the audit found that overall 40% of patients were not given a diagnosis of dementia and 85% of patients under the age of 65 were not given a diagnosis of dementia
Slide #3:
Slide #7
Functional cognitive disorder (FCD)
[Ed: For ICD-11, Dissociative neurological symptom disorder, with cognitive symptoms is coded at 6B60.9 as a child category under parent class: 6B60 Dissociative neurological symptom disorder.]
Slide #25 (My blue highlighting)
Primary care
[Ed: NICE NG127 = Suspected neurological conditions: recognition and referral NICE guideline [NG127] Published date: May 2019 Last updated: July 2019 https://www.nice.org.uk/guidance/ng127]
Slide #26 (My blue highlighting)
MAS triage
Slide #28
Diagnostic and post diagnostic pathway
Slide #29 (My blue highlighting)
FCD Flags
Slide #30
Case study
PDF URL (and attached below): https://www.england.nhs.uk/london/w.../8/2019/07/Final-non-dementia-pathways-V2.pdf
Attachments
Last edited: