Arvo
Senior Member (Voting Rights)
Copied from Deep phenotyping of post-infectious myalgic encephalomyelitis/chronic fatigue syndrome, 2024, Walitt et al
I do not get the impression that this part of the study is an honest, illness- and patientinput-driven look into ME; to me it looks an awful lot like an effort to (further) establish the acceptance of a desired "effort preference"/effort avoidance framework of ME. More tool than find.
Looking at some context, it also doesn't not reassure me that it's not. Walitt called ME a somatoform disorder (a psychiatric disorder where patient's symptoms have no physical basis, and where there is "often a degree of atention-seeking"; the replacement term for hysteria) and sees it through a behavioural lens.
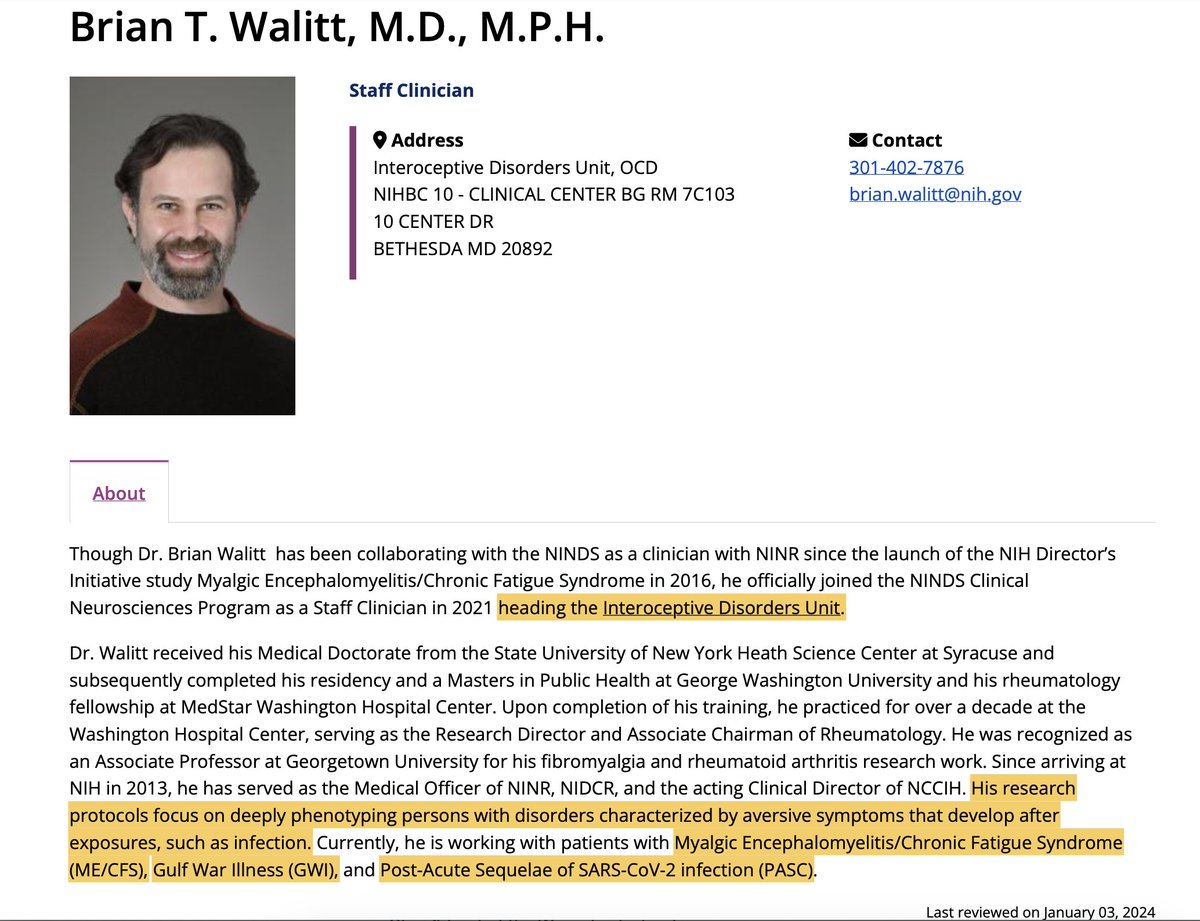
As mentioned elsewhere, "[Walitt's] research protocols focus on deeply phenotyping persons with disorders characterized by aversive symptoms that develop after exposures, such as infection. Currently, he is working with patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), Gulf War Illness (GWI), and Post-Acute Sequelae of SARS-CoV-2 infection (PASC)."(Link)
Disability stemming from disease is not the same at all as "aversive symptoms that develop after exposures".
Like the psychiatrists before him, he is framing ME disability as a tendency to avoid activity, as something patients do instead of what happens to them.
Walitt is also the director of the Introceptive Disorders unit.
(I don't know since when, but gaining this new position might have happened during the ME/CFS study period, see the remark from Paddler, a participant: )
And since 2013 Walitt has (among other functions at the NIH) been the acting Clinical Director of NCCIH - National Center for Complementary and Integrative Health.
Here's the NIH's plan on interoception research: Interoception Research | NCCIH (nih.gov)
So far it's mostly a framework/model; this new presentation looks still quite novel and in its infancy substantiationwise, and the intention is to expand it. And this worries me, as this makes patients tools instead of the exit point. (Interoception will need to justify its existence, and they need to do that by proving that its framework is applicable and useful; firstly by showing how and that interoception plays a role in patients, and then secondly that this can be targeted with treatment -which they intend to pull from "complementary and integrative health approaches" like mindfullness, CBT and nutrition- in a way that is useful and cost-effective.)
Interoception is named as a "top scientific priority" of the NCCIH.
I've nosed through the attached PDF of the NCCIH Strategic Plan FY 2021–2025 (which is from May 2021and interestingly does not mention the word "interoception"once - edited) and it indeed reads like European liaison psychiatry aims and bps ideology in a glossy wrapper. What I've seen looked very, very familiar to me.
Now, going back to the NIH ME/CFS study, this says:
and it aligns nicely with the NCCIH aim of "the integration of complementary and conventional care" and its inetroception info:
"Processes involved in interoception could often serve as therapeutic targets of many complementary and integrative health approaches, including psychological and physical approaches such as meditation, acupuncture, and other manual therapies, as well as nutritional approaches such as natural products."
The way it is presented in the NCCIH plan makes it sound benign and helpful, but for me it sounds like it has a great risk, even intention, of pulling meditation, mindfulness, CBT etc into the place where actual medical treatment should be.
Edited to add:post #688 the next post and post #18 continue on this topic, adding more sources
The two related S4ME threads are:
this, this is the evidence that this was PROBABLY planned beforehand. I had detected the exact same similitude between that part of the paper and Walitt previous statements, they're identical. The results where PROBABLY written even before this study started. Something is very, very wrong with this study
There ¡s another quote by Walitt that seems to be consistent with what he wrote on the latest paper:
"The discordance between the severity of subjective experience and that of objective impairment is the hallmark of somatoform illnesses, such as fibromyalgia and chronic fatigue syndrome"
from this study: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4750385/
I do not get the impression that this part of the study is an honest, illness- and patientinput-driven look into ME; to me it looks an awful lot like an effort to (further) establish the acceptance of a desired "effort preference"/effort avoidance framework of ME. More tool than find.
Looking at some context, it also doesn't not reassure me that it's not. Walitt called ME a somatoform disorder (a psychiatric disorder where patient's symptoms have no physical basis, and where there is "often a degree of atention-seeking"; the replacement term for hysteria) and sees it through a behavioural lens.
As mentioned elsewhere, "[Walitt's] research protocols focus on deeply phenotyping persons with disorders characterized by aversive symptoms that develop after exposures, such as infection. Currently, he is working with patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), Gulf War Illness (GWI), and Post-Acute Sequelae of SARS-CoV-2 infection (PASC)."(Link)
Disability stemming from disease is not the same at all as "aversive symptoms that develop after exposures".
Like the psychiatrists before him, he is framing ME disability as a tendency to avoid activity, as something patients do instead of what happens to them.
Walitt is also the director of the Introceptive Disorders unit.
(I don't know since when, but gaining this new position might have happened during the ME/CFS study period, see the remark from Paddler, a participant: )
I forget the timing but the NIH brought together specialists from various fields to discuss the concept of fatigue a few years after I completed phase 2 of the study. This is where the ideas around interoception were discussed. Apparently Dr Wallit has a new title with the word interoception included.
And since 2013 Walitt has (among other functions at the NIH) been the acting Clinical Director of NCCIH - National Center for Complementary and Integrative Health.
Here's the NIH's plan on interoception research: Interoception Research | NCCIH (nih.gov)
So far it's mostly a framework/model; this new presentation looks still quite novel and in its infancy substantiationwise, and the intention is to expand it. And this worries me, as this makes patients tools instead of the exit point. (Interoception will need to justify its existence, and they need to do that by proving that its framework is applicable and useful; firstly by showing how and that interoception plays a role in patients, and then secondly that this can be targeted with treatment -which they intend to pull from "complementary and integrative health approaches" like mindfullness, CBT and nutrition- in a way that is useful and cost-effective.)
Interoception is named as a "top scientific priority" of the NCCIH.
"Because of its potential importance, research on interoception in the context of complementary and integrative health approaches requires a deeper understanding of the connections between brain and body. In addition, tools and methods to probe interoceptive processes, especially in human subject research, are largely limited to self-reports and a handful of measures such as heart rate variability and skin conductance. An expansion of innovative and quantitative methods to study interoception may significantly enhance our understanding of how interoception works. These new tools and methods may also provide novel insights into how complementary and integrative health approaches may modulate the interoceptive processes and interoceptive clinical outcomes."
What Does Success Look Like?
What Does Success Look Like?
- Expanded understanding of the mechanisms underlying interoception.
- Improved, innovative tools and methods to probe interoceptive processes, especially in human subjects.
- Increased understanding of the impact of specific complementary and integrative health approaches on interoceptive processes.
- Improved understanding of the efficacy and effectiveness of complementary and integrative health approaches on interoception-related clinical outcomes, especially those related to musculoskeletal and visceral pain.
- Build on basic interoceptive pathway studies to investigate mechanisms important for complementary and integrative approaches.
- Expand mechanistic research on interoception involving pain, cardiovascular conditions, and digestive conditions.
- Develop translational and clinical efficacy studies supporting development of new tools to probe interoception in humans and animal models.
- Support natural product research related to interoception involving brain-gut interactions and brain-cardiovascular/immune and brain-endocrine pathways, including both neural and nonneural pathways.
- Support mind and body research involving brain-respiratory (meditation), brain-musculoskeletal (acupuncture/manual therapy, movement-based therapies), brain-cardiovascular, brain-endocrine, and vagal/spinal pathways.
I've nosed through the attached PDF of the NCCIH Strategic Plan FY 2021–2025 (which is from May 2021
It's wrapped in unctuous words and peppered with the familiar buzz words, at first scan the basics are the same. The BPS movement aims to inegrate psychiatry with conventional medicine in order to be able to treat medical issues from a psychiatric angle (CBT); they claim that this way they are treating the "whole person", and are very loudly claiming they are working "evidence-based", based on their own wobbly studies. The NCCIH "has worked to advance the position that evidence-based complementary therapies should be “integrated” with and not used as an “alternative” to conventional medicine." And the subtitle of their plan is: "Mapping a Pathway to Research on Whole Person Health" (and the phrase "whole person" is lavishly peppered throughout the plan).
About those "complementary therapies" it says:
"Complementary and integrative health approaches include a broad range of practices and interventions that may have originated outside of conventional medicine and are gradually being integrated into mainstream health care. These approaches can be classified by their primary therapeutic input, which may be nutritional, psychological, and/or physical. Psychological and/or physical approaches encompass what have been commonly considered mind and body approaches. Commonly used psychological approaches include meditation and cognitive behavioral therapy, while physical approaches include acupuncture, other manual therapies (soft tissue manipulation, massage, spinal and joint manipulation, and related devices), and physical exercise. Some approaches, such as yoga and tai chi, comprise both psychological and physical components."
About those "complementary therapies" it says:
"Complementary and integrative health approaches include a broad range of practices and interventions that may have originated outside of conventional medicine and are gradually being integrated into mainstream health care. These approaches can be classified by their primary therapeutic input, which may be nutritional, psychological, and/or physical. Psychological and/or physical approaches encompass what have been commonly considered mind and body approaches. Commonly used psychological approaches include meditation and cognitive behavioral therapy, while physical approaches include acupuncture, other manual therapies (soft tissue manipulation, massage, spinal and joint manipulation, and related devices), and physical exercise. Some approaches, such as yoga and tai chi, comprise both psychological and physical components."
Now, going back to the NIH ME/CFS study, this says:
Walitt et al said:Therapeutically targeting downstream mechanisms, with exercise, cognitive behavioral therapy, or autonomic directed therapies, may have limited impact on symptom burden, as it would not address the root cause of PI-ME/CFS. However, combination therapy affecting multiple pathways could be considered.
and it aligns nicely with the NCCIH aim of "the integration of complementary and conventional care" and its inetroception info:
"Processes involved in interoception could often serve as therapeutic targets of many complementary and integrative health approaches, including psychological and physical approaches such as meditation, acupuncture, and other manual therapies, as well as nutritional approaches such as natural products."
The way it is presented in the NCCIH plan makes it sound benign and helpful, but for me it sounds like it has a great risk, even intention, of pulling meditation, mindfulness, CBT etc into the place where actual medical treatment should be.
Edited to add:
The two related S4ME threads are:
Last edited: