You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
Aripiprazole - Abilify
- Thread starter Jim001
- Start date
-
- Tags
- abilify aripiprazole
@Jaybee00 - have you posted that tweet on the Abilify thread because Risperidone is, like Abilify, an anti-psychotic?
From Drugbank:
From Drugbank:
Risperidone is a second-generation antipsychotic (SGA) medication used in the treatment of a number of mood and mental health conditions including schizophrenia and bipolar disorder. It is one of the most widely used SGAs. Paliperidone, another commonly used SGA, is the primary active metabolite of risperidone (i.e. 9-hydroxyrisperidone).
Schizophrenia and various mood disorders are thought to be caused by an excess of dopaminergic D2 and serotonergic 5-HT2A activity, resulting in overactivity of central mesolimbic pathways and mesocortical pathways, respectively. Risperidone is thought to reduce this overactivity through inhibition of dopaminergic D2 receptors and serotonergic 5-HT2A receptors in the brain.
Risperidone binds with a very high affinity to 5-HT2A receptors, approximately 10-20 fold greater than the drug's binding affinity to D2 receptors, and carries lesser activity at several off-targets which may responsible for some of its undesirable effects.
Last edited:
Are you seeing many other people trying risperidone with or without amitriptyline? At a first glance, an idea that 'an excess of serotonergic 5-HT2A activity' is involved with (severe) ME/CFS doesn't look very likely to me.
I can't get into X anymore. Does the X thread give any details?
I can't get into X anymore. Does the X thread give any details?
ryanc97
Senior Member (Voting Rights)
I am restarting abilify, planning Mon-Wed 25mg modafinil and Thurs-Fri Abilify 2mg in my attempt to stabilize my brainfog/fatigue until I can go back to working.After being off Abilify for some time now I do worry that for some patients it ´´masks`` cognitive PEM symptoms and thus leads to patients overexerting themselves.
I will say this: both clear brainfog and fatigue. However, abilify for some reason can clear it without the HR/BP pump up, but modafinil cannot. However abilify reduces the effect of modafinil. On Thurs/Fri, I feel very clear headed, much less tired but not as wired like on modafinil.
For example, when I take my BP 3 hours after taking modafinil, i get like 130/90 95. but abilify gets me 125/80 75.
Also this is interesting, I don't seem to get cognitive PEM which I guess I am quite thankful for. On the good days with stimulants, I can think quite decently almost back to my old brain, and I don't seem to get any payback for it.
Last edited:
leokitten
Senior Member (Voting Rights)
I am restarting abilify, planning Mon-Wed 25mg modafinil and Thurs-Fri Abilify 2mg in my attempt to stabilize my brainfog/fatigue until I can go back to working.
I will say this: both clear brainfog and fatigue. However, abilify for some reason can clear it without the HR/BP pump up, but modafinil cannot. However abilify reduces the effect of modafinil. On Thurs/Fri, I feel very clear headed, much less tired but not as wired like on modafinil.
For example, when I take my BP 3 hours after taking modafinil, i get like 130/90 95. but abilify gets me 125/80 75.
Also this is interesting, I don't seem to get cognitive PEM which I guess I am quite thankful for. On the good days with stimulants, I can think quite decently almost back to my old brain, and I don't seem to get any payback for it.
In some of us Abilify can significantly reduce PEM while also increasing energy. Like you said I also feel more like the old me. It's not perfect you can still feel a bit of PEM if you push yourself too hard, but in some of us the improvement is dramatic. I don't get any good effects from modafinil or stimulants, only Abilify.
Rick Sanchez
Senior Member (Voting Rights)
Also this is interesting, I don't seem to get cognitive PEM which I guess I am quite thankful for.
This was something I noticed too.. Massively reduced cognitive. PEM But wasnt sure if it was just down to placebo
I was able to do slightly more cognitively too. But not enough that again. I wasnt sure if it was just down to something like natural fluctuations
I do think Abilify actually might be one of the only things that actually does something. And I think research here might yield important results to understand the nature of MECFS
Still would not recommend the treatment to anyone (a very successful pharma guy I know was worried when I told him I was on it because it had so many side effects). But I think there is enough noise there that it definitely does SOMETHING to affect a decent amount of MECFS patients, and thus make a good research target.
leokitten
Senior Member (Voting Rights)
Its quite interesting. I am hoping doing it 2 days a week basically prevents tolerance.
From my personal experience with LDA since it has such a long half life that skipping days makes little difference compared to daily dosing a lower dose. No matter what steady state dose I have in my system eventually it doesn't work as well and I have to take a break for 4-6 months before it will start working again like before.
Rick Sanchez
Senior Member (Voting Rights)
The anecdotes being so similar with LDA also puts in a different league compared to LDN or whatever other rubbish.
Dont want a big study to see if it works (bc i dnt see it as woking long term, which is also a good argument against trying jt). But a smaller study where you measure what happens to patients. Induce mild to moderate PEM in patients. and see difference before and after LDA.
Should be said I can't recommend anyone trying it. In fact id still .make the argument that people should NOT try LDA. I only did so myself because my parents guilt trip me into treatments all the time and I hadn't considered the possible very serious side affects with LDA that I have since been informed of.
Dont want a big study to see if it works (bc i dnt see it as woking long term, which is also a good argument against trying jt). But a smaller study where you measure what happens to patients. Induce mild to moderate PEM in patients. and see difference before and after LDA.
Should be said I can't recommend anyone trying it. In fact id still .make the argument that people should NOT try LDA. I only did so myself because my parents guilt trip me into treatments all the time and I hadn't considered the possible very serious side affects with LDA that I have since been informed of.
Last edited:
leokitten
Senior Member (Voting Rights)
Given that we just saw from Ponting's recent talk on DecodeME at the ME conference showing most GWAS variants associated with ME involve neuron-related genes, it's again not surprising to me that LDA appears to work really well for some of us. But GWAS also does miss a lot so I don't think it's the entire ME story but it's a good start

Last edited:
leokitten
Senior Member (Voting Rights)
Is the cut off dosage point in mgs for LDA response very black and white for you ?
And is it always at the same dosage you notice improvements?
*NB: I am currently at 1.5 mg LDA with a mild, but varying response on cognitive symptoms, and I’m wondering if I should heighten or stay where I’m at
I've been on GLP-1 meds (tirzepatide) for over two years now and for certain that has had a major modulating and dampening effect on the dopamine system in my brain as well as my dose response to LDA. Before GLP-1s it took only 0.5 mg to get a good and consistent response. Now with GLP-1s it takes 2-3 mg to get a response and it's not the same as before. There's been a lot of research showing GLP-1 meds effect on the mesocorticolimbic system
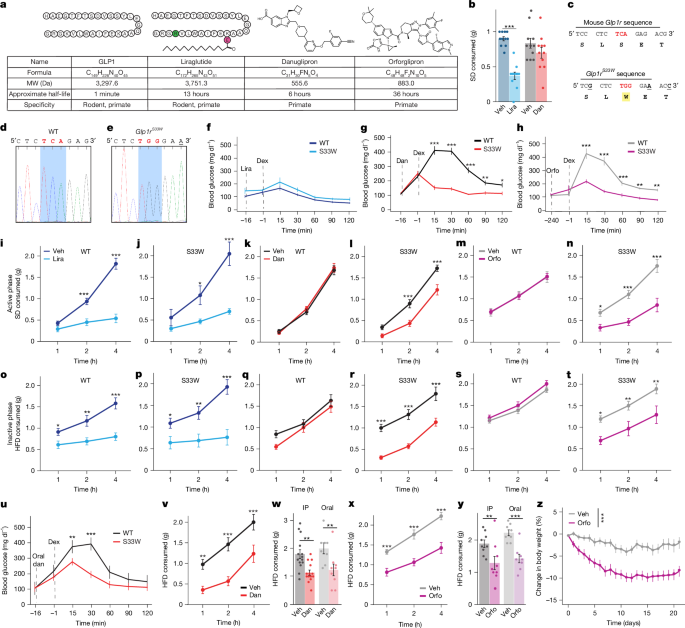
A brain reward circuit inhibited by next-generation weight-loss drugs in mice - Nature
Humanized glucagon-like peptide 1 receptor (GLP1R) mouse models are used to investigate the neural circuitry through which small-molecule GLP1R agonists modulate feeding, with implications for how these orally delivered weight-loss drugs engage brain reward circuits.
 www.nature.com
www.nature.com
Curbing the appetites and restoring the capacity for satisfaction: The impact of GLP-1 agonists on the reward circuitry
Hedonic eating is controlled by dopamine neurons that oppose GLP-1R satiety
Last edited: