A fatigue clinic in Holland using CCS model based on Jo Nijs’work. Google translation below from their page:
Physiotherapy in patients with chronic fatigue syndrome
ME / CFS and fibromyalgia are unexplained, no cause is known. Patients have especially severe fatigue and many other complaints that only get worse by physical exertion; the immune system is (further) disrupted.
The latter is not seen to the extent with other disorders, as physical effort often has a 'complaining-damping' effect.
Patients often have unrealistic expectations and / or incorrect beliefs about the origin of their chronic complaints, the usefulness of rest and the fear of movement. Stress causes extra stress, sleep is an important point of interest (a scientific study of 350 sleep study results among our fatigue patients gave a significant disturbance to the effectiveness of sleep at 100%).
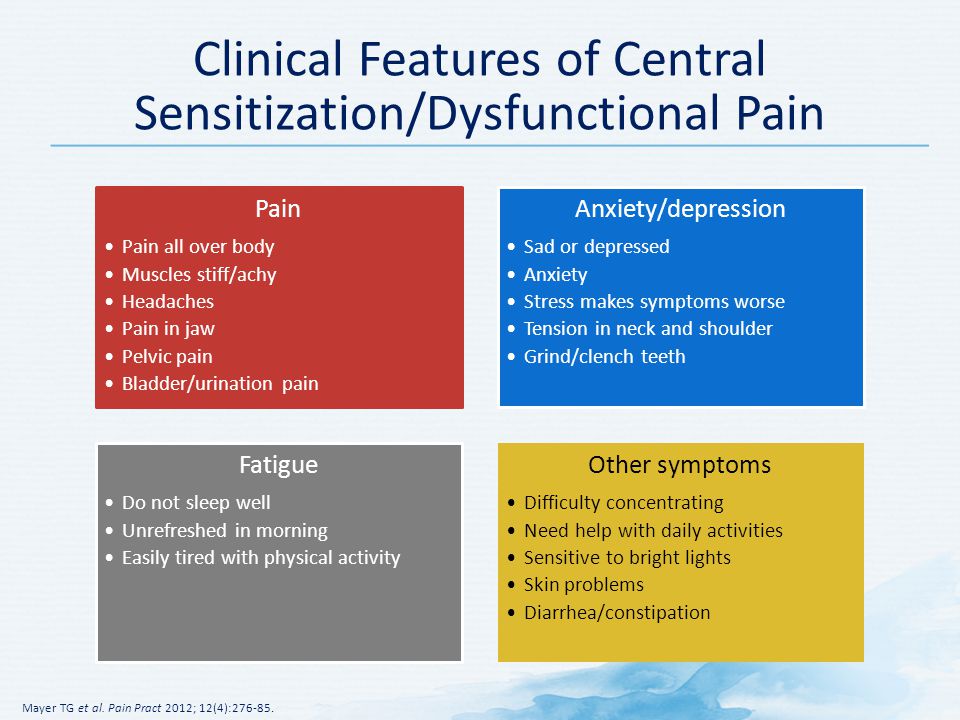
In the treatment by the psychosomatic physical therapist, we refer to the explanatory model of Prof. Dr. Jo Nijs (VU Brussels): the mechanism of central sensitization (named after the patient: 'hypersensitive nervous system'). The information supply of the nervous system is disrupted. Not activating the damping system gives increased sensitivity of fatigue / pain signal or disturbing the sensitivity of sensory signals. Therefore, management of activities and exercise must be treated very carefully. Together with the ME / CVS Foundation these are set out in a folder.
It seems a paradox: exercise gives an increase in symptoms versus it is important to move. But it is only the "exaggerated" forms of physical exertion that lead to malaise (such as performing a (sub) maximum exercise test or long-term work in the garden). Therapy must be tailored to the possibilities: with low intensity and short periods of exertion, alternated with rest breaks. This requires a great deal of expertise from the therapists, and in the case of Fatigue & Pain Center, therapists and patients are supported by the Activity and Motion Weigher.
Measuring is knowing
With the help of the "Beweegweger", which makes the load on the activity measurable, the patient learns to build up the loadability in a responsible manner. Prior to this, a study is taking place with the Sensewear, which measures, among other things, metabolism throughout the day. The motion scale then calculates how many METs (metabolic equivalent of a task) is an operation. The physiotherapist and patient thus have insight into whether the patient advances in energy. The ultimate goal is to increase the load capacity. A second measurement with Sensewear objectifies the result.
https://vermoeidheidenpijncentrum.n...herapie-bij-chronisch-vermoeidheids-syndroom/
 )
)