Action for M.E. investigated the services provided in the UK under the NHS through the Primary Care Trusts in England and Wales, and published the results in their Spring 2012 magazine (issue 79). They found that only 54% of those trusts were able to state that they actually commission specialist M.E. services, and just 20% stated that they provided some form of home visit for those too ill to travel. I saw my specialist in 2001, and that was outside the NHS.
Even those patients lucky enough to live in an area that offers support services and well enough to attend, still face the lottery of how thoroughly the further diagnosis is carried out. Unlike the comprehensive testing carried out by Newcastle, many (most?) patients have perhaps a twenty-minute interview with a specialist, and are then passed on to a team trained to deliver CBT/GET.
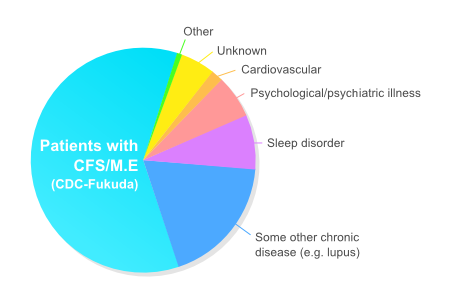
Both of the main ME support organizations in the UK (MEA, AfME) use the estimate that there are 250,000 people with the diagnosis of ME/CFS in the UK. If we use the figure provided by Newcastle that 40% of those given that provisional diagnosis of ME/CFS turn out not to have ME/CFS, but something else, this gives us an estimate of 150,000 people who actually have ME in the UK, while 100,000 have an incorrect diagnosis. Allowing for poorer diagnosis in the past, it is likely that this is more likely to balance out at around 125,000 each. This would be similar to the estimate given by Nacul et al. of there being about 0·19%, or 118,000 actually having ME/CFS according to CDC 1994 criteria.
125,000 is a worryingly large number of people carrying a diagnosis of ME/CFS, who potentially have another, often more treatable illness.
Research from Newcastle by Hoad et al. suggests that a significant proportion of people with a preliminary diagnosis of ME/CFS suffer from Postural Orthostatic Tachycardia Syndrome. For some this may be their main problem: for others it may be just one factor in their illness. We need more evidence to determine how widespread this is, and this needs to be a part of the diagnostic process. This syndrome is explored more fully by Spence and Stewart, or there is a more everyday description from the Telegraph.
The public perception of ME/CFS can be confused by including people who have been diagnosed wrongly as having ME/CFS and who find a cure appropriate to their own different illness. Patients deserve faster and more accurate diagnosis.
A major concern as far as policy decisions are concerned is that many of the studies which inform current policy decisions were carried out when there were far fewer specialists. According to the earlier Newcastle CFS Service report mentioned above, only 36% of patients referred to them in 2007 actually had ME/CFS. If that level of error is even slightly indicative of the unreliability of provisional diagnosis of ME/CFS in earlier years, it casts grave doubt on many of the earlier studies that form the basis of our current policies.
As an example, consider how a study by Harvey et al. in 2007 which reinforced the interpretation of ME/CFS as having strong psychological underpinnings, considered the possible relationship between prior psychiatric disorder and chronic fatigue. This paper actually used self-reported ME/CFS: patients were not actually assessed for having ME/CFS; they simply recorded that they either had been told that they had ME/CFS or felt that they had it. Such reports cannot continue to be authoritative.
Access to specialist care should be made a priority for all people suspected to have ME/CFS because accurate and prompt diagnosis is essential to rational compassionate care. Whether provided through the specialist or through a GP or internist, the basic services such as those provided in the PACE trial as Specialist Medical Care – pain, sleep, and depression support as indicated – should be provided to ME/CFS patients as a matter of course.
summary more
|