For a brief description of the four different sets of criteria for ME/CFS go to the wikipedia entry. For further details of the CDC/Fukuda, London and Canadian Criteria, click here.
It is often argued that post-exertional fatigue is an important marker for ME, and that the Canadian Criteria best represent that illness. This conflict between definitions needs to be tackled. A recent study by Nacul et. al. undertaken as part of the ME/CFS Observatory Research Programme, looking at the functional status of people with ME, concluded that "the fact that the scores of cases meeting the Canadian criteria were consistently lower than those not meeting the criteria further suggests that diagnosis specificity is related to disease severity, and that diagnostic criteria such as the Canadian may be more appropriate for research studies investigating risk factors and disease biomarkers". If we were to use their figures from a related study, that could translate into approximately only a third of the patients in the PACE trial satisfying the Canadian Criteria - but of course, that is speculative.
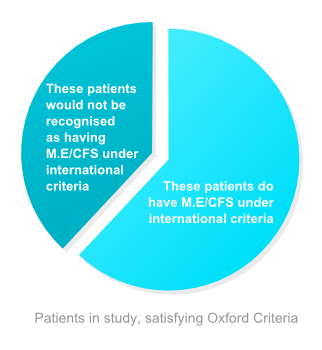
We also need to determine the nature of the illness(es?) classified as ME/CFS under the Oxford Criteria that would not be recognised as ME/CFS under the other criteria (38% of the PACE trial), as these patients should not be excluded from medical research.
A major part of the problem revolves around the way in which "fatigue" plays an important role in naming and specifying the illness. There are a range of other illnesses that have chronic fatigue as a severe consequence, such as heart disease and liver disease, but they do not carry the label CF/Heart Disease or CF/Liver Disease, and this irregularity for ME/CFS is both a source of confusion amongst the public, and a cause of frustration amongst the patients: the technical difference between CF and CFS is too academic for most people to appreciate. For clarity – and accuracy – fatigue needs to be seen as a result of having ME rather than defining the illness.
There have been many conditions in the past that have been renamed both for reasons of accuracy and of perception. This illness needs to be renamed, and the report of the CFS/ME group touches on this in their recommendations in Chapter 6. In the meantime, it seems sensible to adopt the CDC/Fukuda suggestion that those people who experience long-term fatigue for unknown reasons and who do not satisfy the CDC criteria should be classified as having unexplained/ideopathic chronic fatigue (dropping the "Syndrome" ). In that case it would be confusing for the general public if ME/CFS were to continue to be used for those who do satisfy the criteria: either ME alone should be used, or a suitably clear label devised.
A study by van Kessel et al. on the use of CBT for Multiple Sclerosis Fatigue found much greater improvements in fatigue levels as measured by the Chalder scale than was the case in the PACE trial (from 21 to 8 vs 28 to 21). In a study on the use of CBT in rheumatoid arthritis, Hewlett, using the Multi-dimensional Assessment of Fatigue and the Visual Analogue Scale, found proportionately slightly smaller changes (than PACE) in fatigue levels. These studies are not robustly comparable with studies on ME/CFS, but they put the ME results firmly in the group of major illnesses for which great fatigue is a consequence.
Towards the end of a report by the Newcastle NHS CFS Service (the findings of which are covered in section 4), an interesting case is made for setting up Fatigue Clinics, rather like Pain Clinics, that are not devoted to any one particular illness. This sort of approach would free research to study ME itself, and put it on a par with other fatigue-associated illnesses, removing a lot of the confusion.
For a fuller account of the differences between the criteria and the way in which this affects studies, please see further details.
Stepping back from the situation, and looking back at the history of ME/CFS, it is obvious that this lack of agreed definition lies at the core of the disagreements between the various factions. The psychologists and psychiatrists, clearly concerned about the increasing number of people suffering from chronic fatigue caused by social, work or psychological factors, devised therapies to help the situation. At the same time a different group of doctors were experiencing epidemic-type spreads of an illness for which profound fatigue was a major result. Through overlapping definitions and nomenclature, and a regrettable tendency to arrive at a diagnosis through a lack of alternative diagnosis, these two fundamentally different phenomena seemed to merge both in the eye of the public and, regrettably, in many areas of the medical profession. There really is no excuse for such sloppy, unscientific thinking to continue.
We are very pleased that the recent report defining International Consensus Criteria for ME has come out so strongly with a way forward with to tackle this problem.
|